T e x a s De pa rt m e nt Of I nsura nc e
Division of Workers’ Compensation
Chief Clerk of Proceedings
7551 Metro Center Dr. Ste.100 • MS-35 Austin, TX 78744-1609
(512) 804-4010 (512) 804-4011 fax www.tdi.texas.gov
DWC Claim#
Carrier Claim#
Send the completed form to this address.
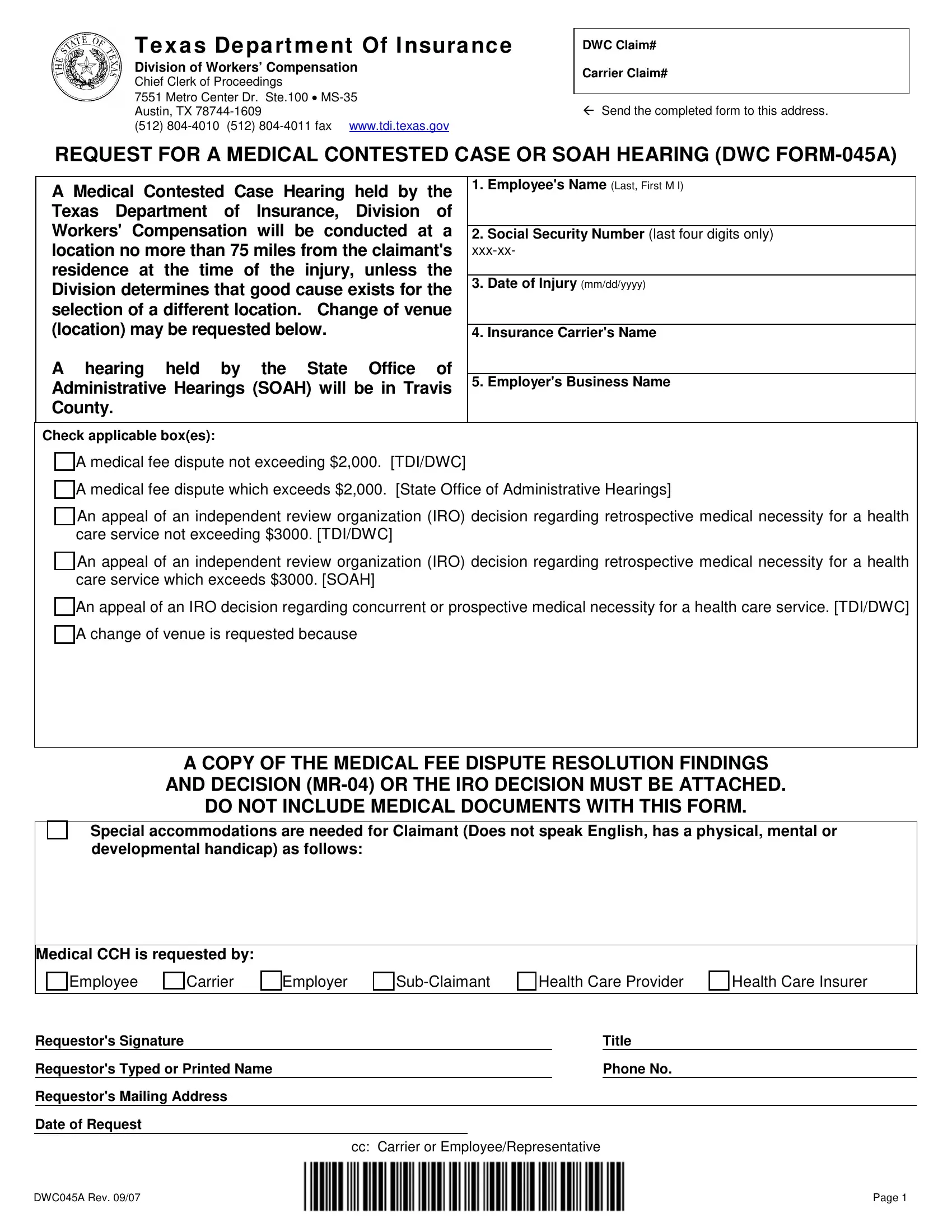
REQUEST FOR A MEDICAL CONTESTED CASE OR SOAH HEARING (DWC FORM-045A)
A Medical Contested Case Hearing held by the Texas Department of Insurance, Division of Workers' Compensation will be conducted at a location no more than 75 miles from the claimant's residence at the time of the injury, unless the Division determines that good cause exists for the selection of a different location. Change of venue (location) may be requested below.
A hearing held by the State Office of Administrative Hearings (SOAH) will be in Travis County.
Check applicable box(es):
1.Employee's Name (Last, First M I)
2.Social Security Number (last four digits only) xxx-xx-
3.Date of Injury (mm/dd/yyyy)
4.Insurance Carrier's Name
5.Employer's Business Name
A medical fee dispute not exceeding $2,000. [TDI/DWC]
A medical fee dispute which exceeds $2,000. [State Office of Administrative Hearings]
An appeal of an independent review organization (IRO) decision regarding retrospective medical necessity for a health care service not exceeding $3000. [TDI/DWC]
An appeal of an independent review organization (IRO) decision regarding retrospective medical necessity for a health care service which exceeds $3000. [SOAH]
An appeal of an IRO decision regarding concurrent or prospective medical necessity for a health care service. [TDI/DWC] A change of venue is requested because
A COPY OF THE MEDICAL FEE DISPUTE RESOLUTION FINDINGS
AND DECISION (MR-04) OR THE IRO DECISION MUST BE ATTACHED.
DO NOT INCLUDE MEDICAL DOCUMENTS WITH THIS FORM.
Special accommodations are needed for Claimant (Does not speak English, has a physical, mental or developmental handicap) as follows:
Medical CCH is requested by:
Carrier |
|
Employer |
|
Sub-Claimant |
|
Health Care Provider |
|
Health Care Insurer |
Requestor's Signature |
|
|
|
Title |
Requestor's Typed or Printed Name |
|
|
|
Phone No. |
Requestor's Mailing Address |
|
|
|
|
Date of Request |
|
|
|
|
|
cc: Carrier or Employee/Representative |
DWC045A Rev. 09/07 |
|
|
|
Page 1 |
DWC FORM-045A
Request for a Medical Contested Case or SOAH Hearing
A party to a claim is entitled to file a Request for a Medical Contested Case Hearing (DWC FORM-045A) with the Chief Clerk of Proceedings of the Texas Department of Insurance, Division Workers' Compensation, in order to resolve disputed medical issues. The Chief Clerk of Proceedings of the Texas Department of Insurance, Division of Workers' Compensation, will schedule the conference. If the hearing is to be held by the Division of Workers' Compensation, it will be conducted at a site no more than 75 miles from the claimant's residence, at the time of the injury, unless the Division determines that good cause exists for the selection of a different location. If the hearing is to be held by the State Office of Administrative Hearings, it will be held in Travis County.
If the requestor is an Employee, a Health Care Provider, a Carrier, an Employer or a Health Care Insurer, the appropriate block should be checked; if none of these apply, then the Sub-Claimant block should be checked.
The DWC FORM-045A is considered filed when received by the Chief Clerk of Proceedings of the Texas Department of Insurance, Division of Workers' Compensation or when personally delivered to the Texas Department of Insurance, Division of Workers' Compensation. The form should be filed with the Chief Clerk of Proceedings. Failure to file the form with the Chief Clerk may delay processing.
NOTE: With few exceptions, you are entitled, on request, to be informed about the information that the Division collects or maintains about you and your workers’ compensation claim. Under §552.021 and 552.023 of the Texas Government Code, you are entitled to receive and review the information. Under §559.004 of the Texas Government Code you are entitled to have the Division correct information the Division creates about you or your workers’ compensation claim that is incorrect. For more information, call the local Division Field Office at 1-800-252-7031.
DWC045A Rev. 09/07 |
Instructions |