
In case you want to fill out form20employee, there's no need to download any applications - simply give a try to our PDF tool. Our tool is continually developing to deliver the very best user experience attainable, and that is thanks to our commitment to continuous improvement and listening closely to user opinions. By taking some easy steps, it is possible to start your PDF journey:
Step 1: Click the "Get Form" button in the top section of this webpage to access our PDF tool.
Step 2: Once you start the file editor, you will notice the form prepared to be filled out. Other than filling in various blank fields, you could also perform many other actions with the PDF, that is putting on your own textual content, editing the initial text, adding graphics, placing your signature to the document, and more.
This PDF form will need specific information; to guarantee accuracy, be sure to take into account the following tips:
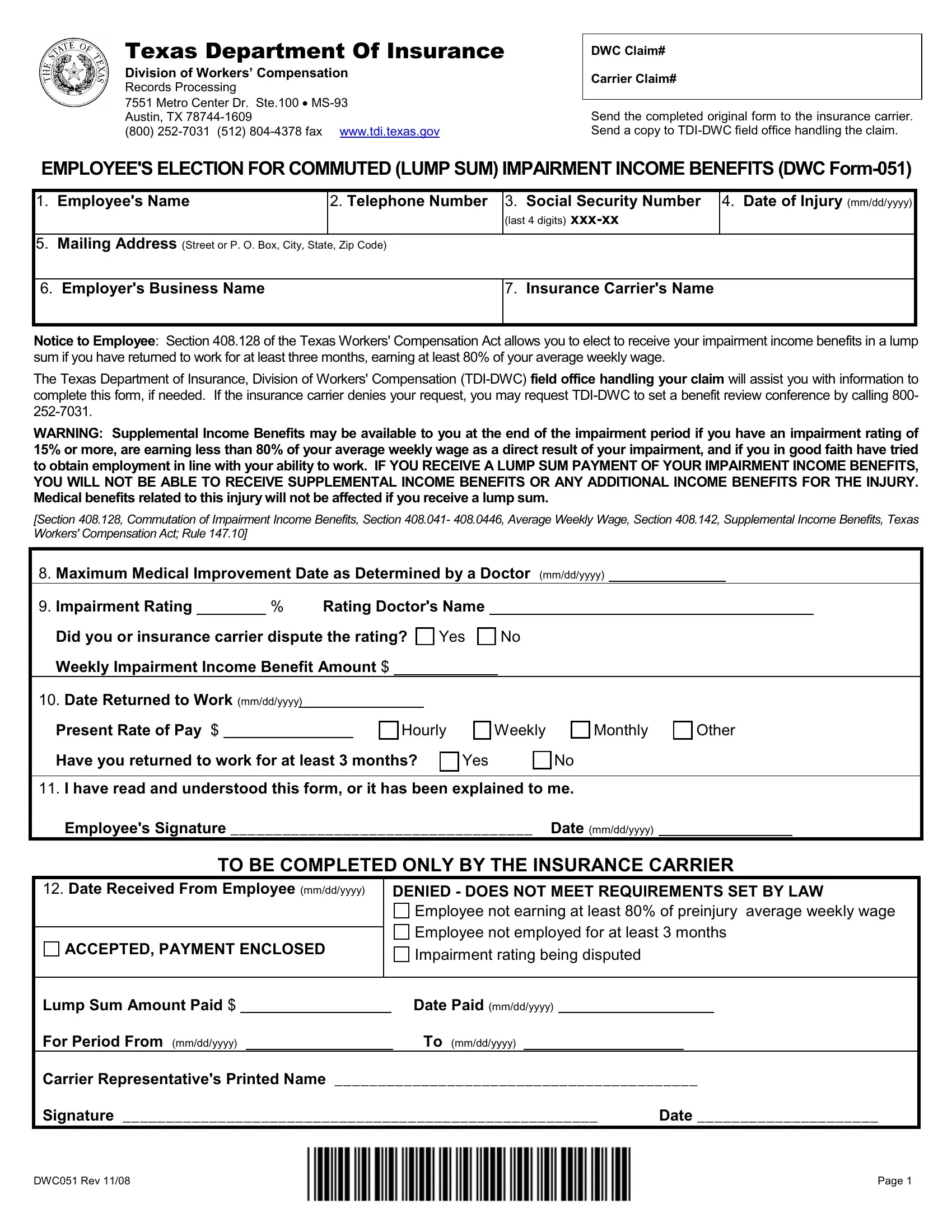
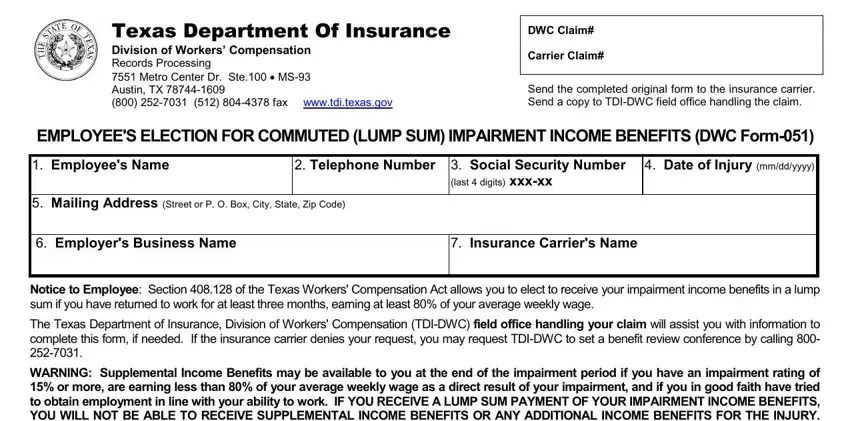
1. Complete the form20employee with a group of necessary blank fields. Consider all the information you need and be sure absolutely nothing is missed!
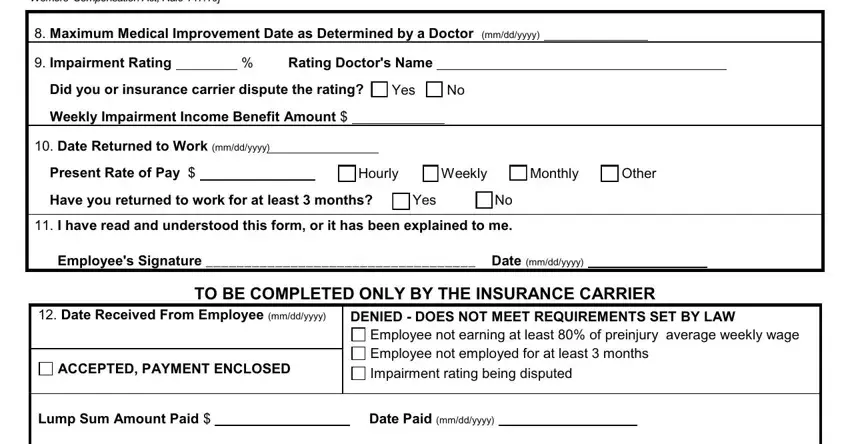
2. When the previous section is completed, you have to add the required specifics in Section Commutation of Impairment, Maximum Medical Improvement Date, Impairment Rating Rating, Did you or insurance carrier, Yes, Weekly Impairment Income Benefit, Date Returned to Workmmddyyyy, Present Rate of Pay, Hourly, Weekly, Monthly, Other, Have you returned to work for at, Yes, and I have read and understood this so you're able to go further.
3. This third step is going to be hassle-free - fill out all the empty fields in from, the, website, field, office, downloading, and Who may use this form to elect in order to complete the current step.
Lots of people generally make mistakes when filling out field in this section. Don't forget to reread whatever you enter right here.
Step 3: Prior to moving on, make certain that blanks were filled in right. Once you are satisfied with it, click “Done." After starting a7-day free trial account at FormsPal, you will be able to download form20employee or send it through email immediately. The PDF document will also be readily available via your personal account menu with all of your adjustments. FormsPal guarantees your data confidentiality by using a secure method that in no way saves or distributes any type of sensitive information involved in the process. Rest assured knowing your documents are kept protected every time you use our services!