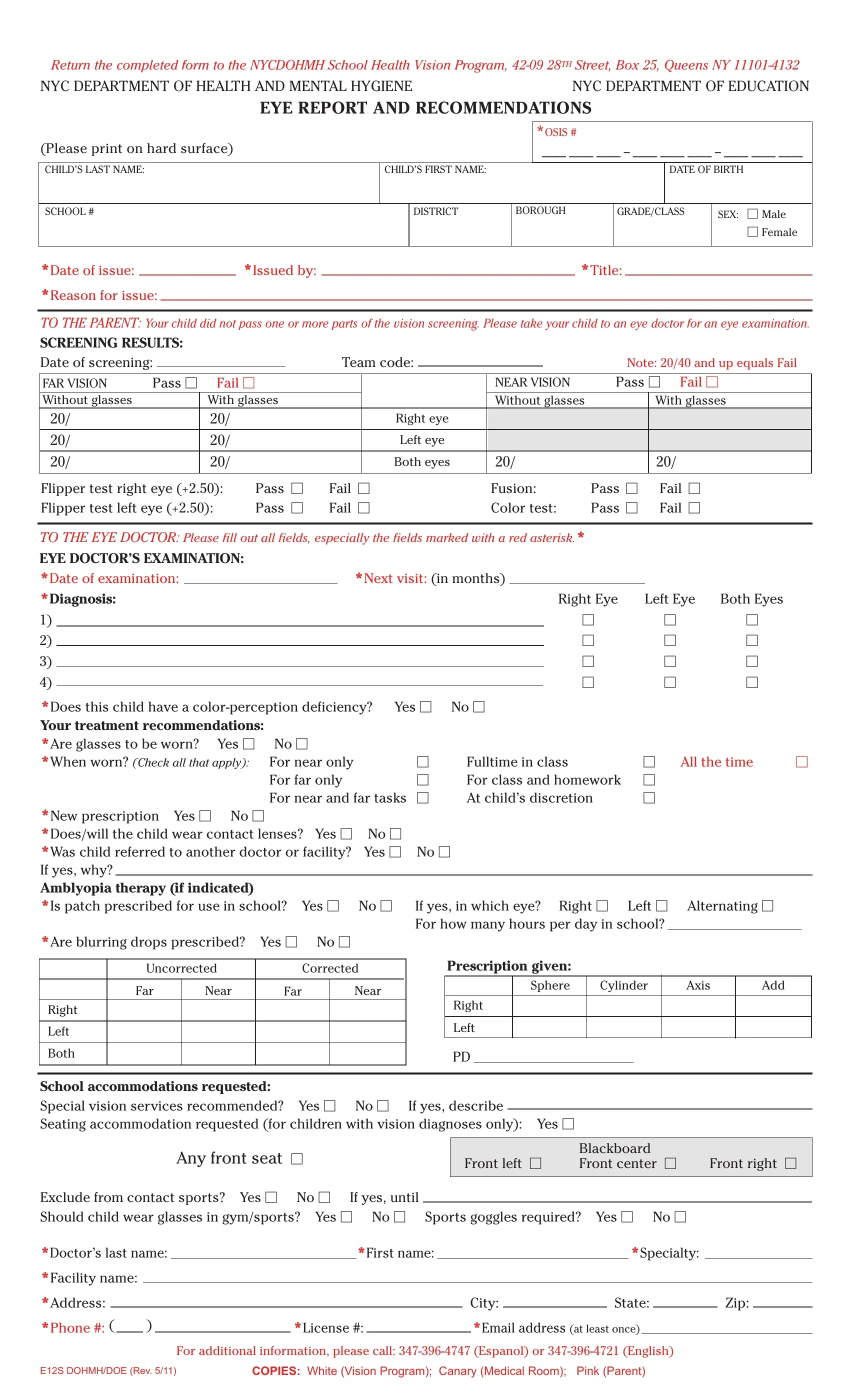
The E12S Dohmh Doe form is a crucial document designed to facilitate communication between the school system and healthcare professionals regarding a child's vision health. It's usually filled out when a child does not pass a vision screening conducted at their school. This form serves multiple purposes: to inform parents about their child's failing vision screening results, guide them in seeking further eye examination from an eye doctor, and relay the doctor's examination findings and recommendations back to the school. The document is comprehensive, covering screening results, eye doctor's examination, diagnosis, treatment recommendations, including whether glasses or contact lenses are needed, and if any specific accommodations are required at school to support the child's vision needs. Additionally, it provides information on special services for children with very low vision offered by the New York City Department of Education, aiming to maintain students' access to education despite vision impairments. The completed form must be returned to the NYCDOHMH School Health Vision Program, highlighting the collaboration between the New York City Department of Health and Mental Hygiene and the Department of Education to ensure children receive the necessary support for their vision health.
| Question | Answer |
|---|---|
| Form Name | Form E12S Dohmh Doe |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | e12s form, 28TH, e12s form doe, OSIS |
Return the completed form to the NYCDOHMH School Health Vision Program,
NYC DEPARTMENT OF HEALTH AND MENTAL HYGIENE |
NYC DEPARTMENT OF EDUCATION |
EYE REPORT AND RECOMMENDATIONS
(Please print on hard surface)
*OSIS #
____ ____ ____ – ____ ____ ____ – ____ ____ ____
CHILD’S LAST NAME:
CHILD’S FIRST NAME:
DATE OF BIRTH
SCHOOL #
DISTRICT
BOROUGH
GRADE/CLASS
SEX: Male
Female
*Date of issue: |
|
*Issued by: |
|
*Title: |
|
|
*Reason for issue:
TO THE PARENT: Your child did not pass one or more parts of the vision screening. Please take your child to an eye doctor for an eye examination.
SCREENING RESULTS: |
|
|
|
|
|
|
|
|
||
Date of screening: |
|
|
Team code: |
|
|
|
Note: 20/40 and up equals Fail |
|||
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
||
FAR VISION |
Pass |
Fail |
|
|
|
NEAR VISION |
Pass Fail |
|||
Without glasses |
|
|
With glasses |
|
|
|
Without glasses |
|
With glasses |
|
20/ |
|
|
20/ |
|
Right eye |
|
|
|
|
|
20/ |
|
|
20/ |
|
Left eye |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20/ |
|
|
20/ |
|
Both eyes |
20/ |
|
|
20/ |
|
|
|
|
|
|
|
|
|
|
|
|
Flipper test right eye (+2.50): |
Pass |
Fail |
Fusion: |
Pass |
Fail |
|
|||||
Flipper test left eye (+2.50): |
Pass |
Fail |
Color test: |
Pass |
Fail |
|
|||||
|
|
|
|
|
|
|
|
||||
TO THE EYE DOCTOR: Please fill out all fields, especially the fields marked with a red asterisk.* |
|
|
|||||||||
EYE DOCTOR’S EXAMINATION: |
|
|
|
|
|
|
|
|
|
||
*Date of examination: |
|
|
|
*Next visit: (in months) |
|
|
|
|
|||
|
|
|
|
|
|
|
|||||
*Diagnosis: |
|
|
|
|
|
|
Right Eye |
Left Eye |
Both Eyes |
||
1) |
|
|
|
|
|
|
|
|
|||
2) |
|
|
|
|
|
|
|
|
|||
3) |
|
|
|
|
|
|
|
|
|||
4) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||||
*Does this child have a |
Yes |
No |
|
|
|
Your treatment recommendations: |
|
|
|
|
|
*Are glasses to be worn? Yes |
No |
|
|
|
|
*When worn? (Check all that apply): |
For near only |
Fulltime in class |
All the time |
||
|
For far only |
For class and homework |
|
||
|
For near and far tasks |
At child’s discretion |
|
||
*New prescription Yes No |
|
|
|
|
|
|
*Does/will the child wear contact lenses? |
Yes |
No |
|
|
|
|
*Was child referred to another doctor or facility? |
Yes |
No |
||||
If yes, why? |
|
|
|
|
|
|
Amblyopia therapy (if indicated) |
|
|
|
|
|
|
*Is patch prescribed for use in school? Yes |
No |
If yes, in which eye? Right Left Alternating |
||||
*Are blurring drops prescribed? Yes |
No |
|
For how many hours per day in school? |
|
|
|
|
|
|
|
|||
Uncorrected |
|
Corrected |
|
|
|
|
|
Far |
Near |
Far |
Near |
Right
Left
Both
Prescription given:
Sphere |
Cylinder |
Axis |
Add |
Right
Left
PD
School accommodations requested:
Special vision services recommended? Yes No If yes, describe
Seating accommodation requested (for children with vision diagnoses only): Yes
Any front seat
|
Blackboard |
|
Front left |
Front center |
Front right |
Exclude from contact sports? Yes |
No If yes, until |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Should child wear glasses in gym/sports? Yes No |
Sports goggles required? |
Yes |
No |
||||||||||||||||||
*Doctor’s last name: |
|
|
*First name: |
|
|
|
|
|
|
*Specialty: |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
*Facility name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
*Address: |
|
|
|
|
|
|
|
|
|
|
City: |
|
|
State: |
|
|
Zip: |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
*Phone #: ( |
|
) |
|
|
*License #: |
|
|
|
|
*Email address (at least once) |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
For additional information, please call:
E12S DOHMH/DOE (Rev. 5/11) |
COPIES: White (Vision Program); Canary (Medical Room); Pink (Parent) |

PLEASE SEND ALL COMPLETED FORMS TO:
School Health Vision Program
Queens, NY
If you have questions about the form, please call one of the
following numbers:
If your child has ver y low vision, he or she may be eligible for special services provided by the New York City Department of Education.
Educational Vision Services
The New York City Public Schools provide specialized educational services for students who are blind or visually impaired. Students are eligible if their
●Braille
●Large print reading materials
●Training with low vision devices
●Specialized adaptive computer technology
●Instruction in other skills to attain literacy in:
●reading
●writing
●mathematics
●sciences
●computers
●Instruction in orientation and mobility for independence in travel
●Bus transportation, if needed.
For further information contact:
Educational Vision Services
400 First Avenue, 7th Floor
New York, NY 10010
E12S DOHMH/DOE (Rev. 5/11)