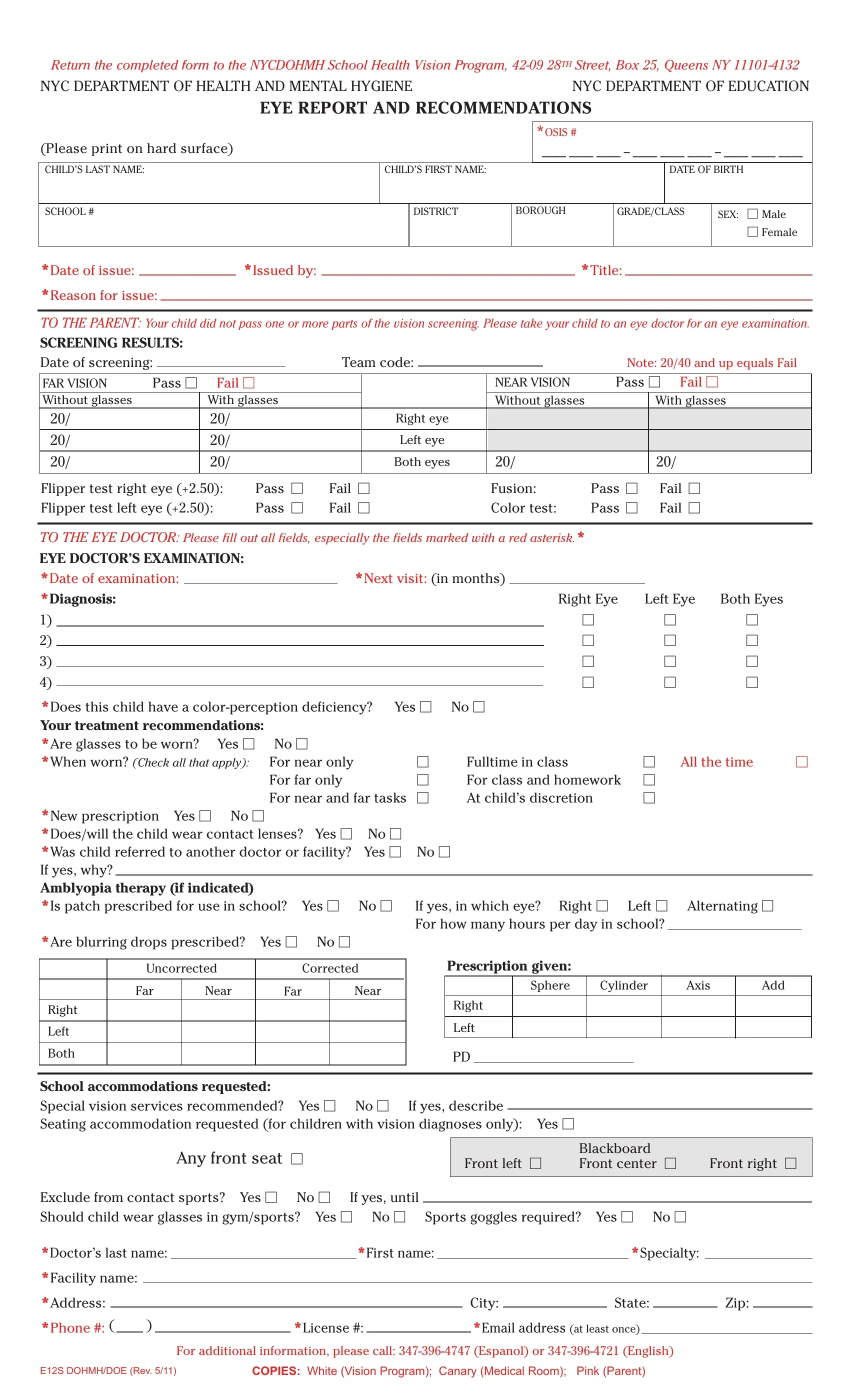
The E12S Dohmh Doe form is a crucial document designed to facilitate communication between the school system and healthcare professionals regarding a child's vision health. It's usually filled out when a child does not pass a vision screening conducted at their school. This form serves multiple purposes: to inform parents about their child's failing vision screening results, guide them in seeking further eye examination from an eye doctor, and relay the doctor's examination findings and recommendations back to the school. The document is comprehensive, covering screening results, eye doctor's examination, diagnosis, treatment recommendations, including whether glasses or contact lenses are needed, and if any specific accommodations are required at school to support the child's vision needs. Additionally, it provides information on special services for children with very low vision offered by the New York City Department of Education, aiming to maintain students' access to education despite vision impairments. The completed form must be returned to the NYCDOHMH School Health Vision Program, highlighting the collaboration between the New York City Department of Health and Mental Hygiene and the Department of Education to ensure children receive the necessary support for their vision health.
| Question | Answer |
|---|---|
| Form Name | Form E12S Dohmh Doe |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | e12s form, 28TH, e12s form doe, OSIS |
