
form ee download can be filled in online very easily. Simply use FormsPal PDF editor to do the job in a timely fashion. Our team is aimed at making sure you have the best possible experience with our editor by consistently adding new capabilities and enhancements. With all of these updates, working with our editor gets better than ever before! To start your journey, consider these basic steps:
Step 1: First, access the pdf editor by clicking the "Get Form Button" above on this webpage.
Step 2: With our online PDF editing tool, you can actually accomplish more than simply complete blank fields. Try all the functions and make your documents seem professional with customized text put in, or optimize the original input to perfection - all that comes with an ability to add just about any pictures and sign the file off.
It is actually easy to finish the form adhering to our helpful tutorial! Here is what you need to do:
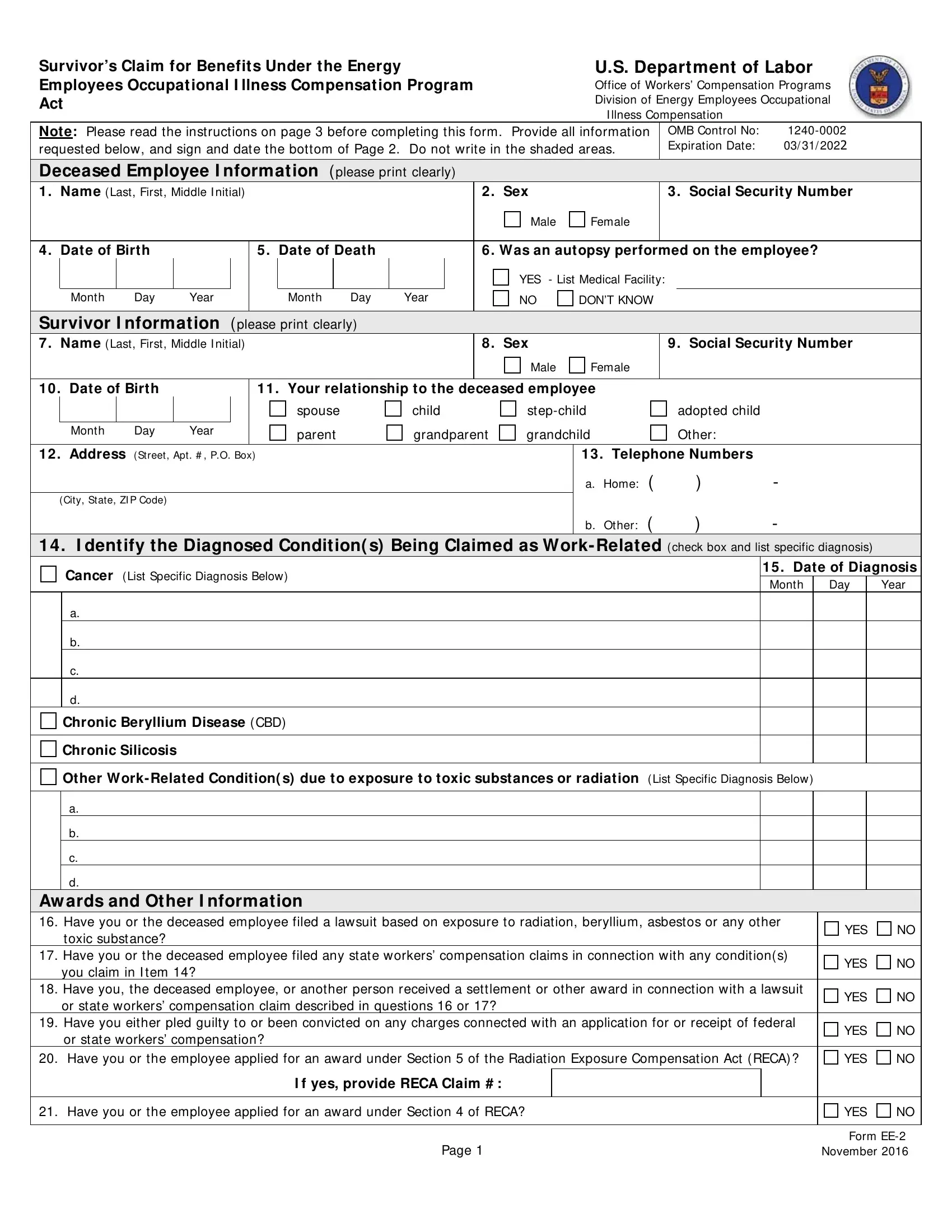
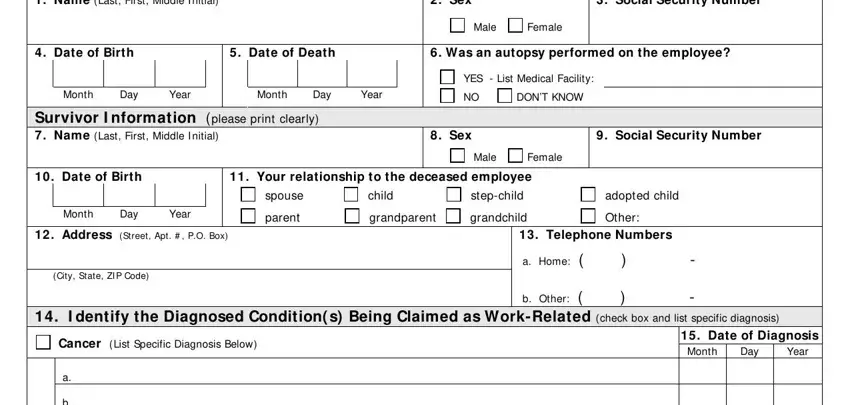
1. While submitting the form ee download, make certain to complete all of the necessary fields within the relevant section. This will help to hasten the work, allowing for your information to be handled swiftly and properly.
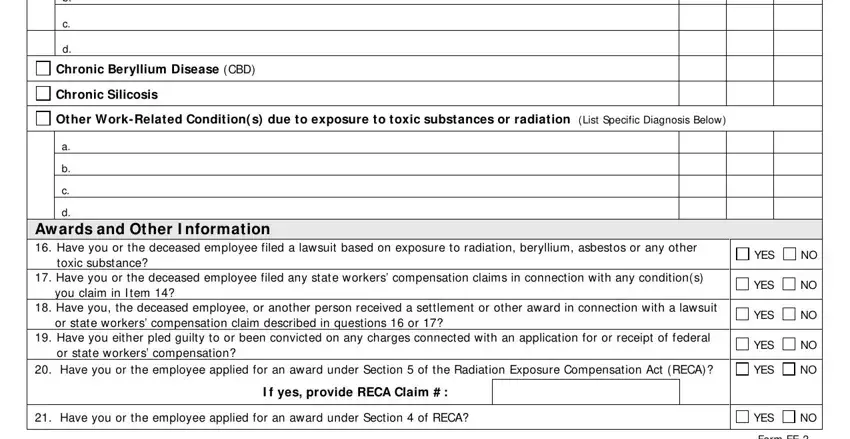
2. After this section is done, go to type in the applicable details in these - Chronic Beryllium Disease CBD, Chronic Silicosis, Other WorkRelated Condition s due, Aw ards and Other I nformation, toxic substance, Have you or the deceased employee, you claim in I tem, Have you the deceased employee or, or state workers compensation, Have you either pled guilty to or, or state workers compensation, YES, YES, YES, and YES.
3. In this specific part, look at Name, Relationship to the deceased, Address, Phone Numbers, Home, Other, Home, Other, Home, Other, Home, Other, Home, Other, and Home. Every one of these are required to be filled in with greatest awareness of detail.
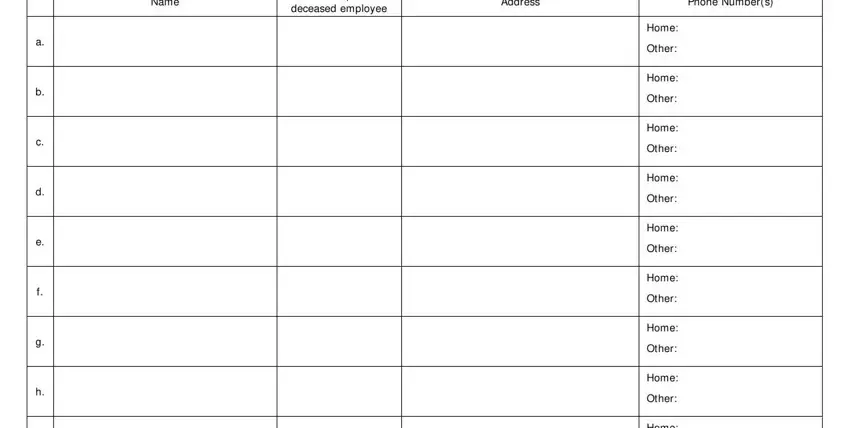
People who work with this document frequently get some things incorrect while completing Other in this section. Ensure that you re-examine whatever you type in here.
4. This particular subsection arrives with all of the following fields to consider: Home, Other, Home, Other, Survivor Declaration Any person, Resource Center Date Stamp, Claimant Signature, Date, Form EE November, and Page.
Step 3: Proofread all the information you've entered into the blanks and then click on the "Done" button. Grab your form ee download after you sign up at FormsPal for a free trial. Quickly gain access to the pdf form from your FormsPal account, along with any modifications and adjustments all kept! Here at FormsPal.com, we strive to guarantee that all of your details are kept secure.