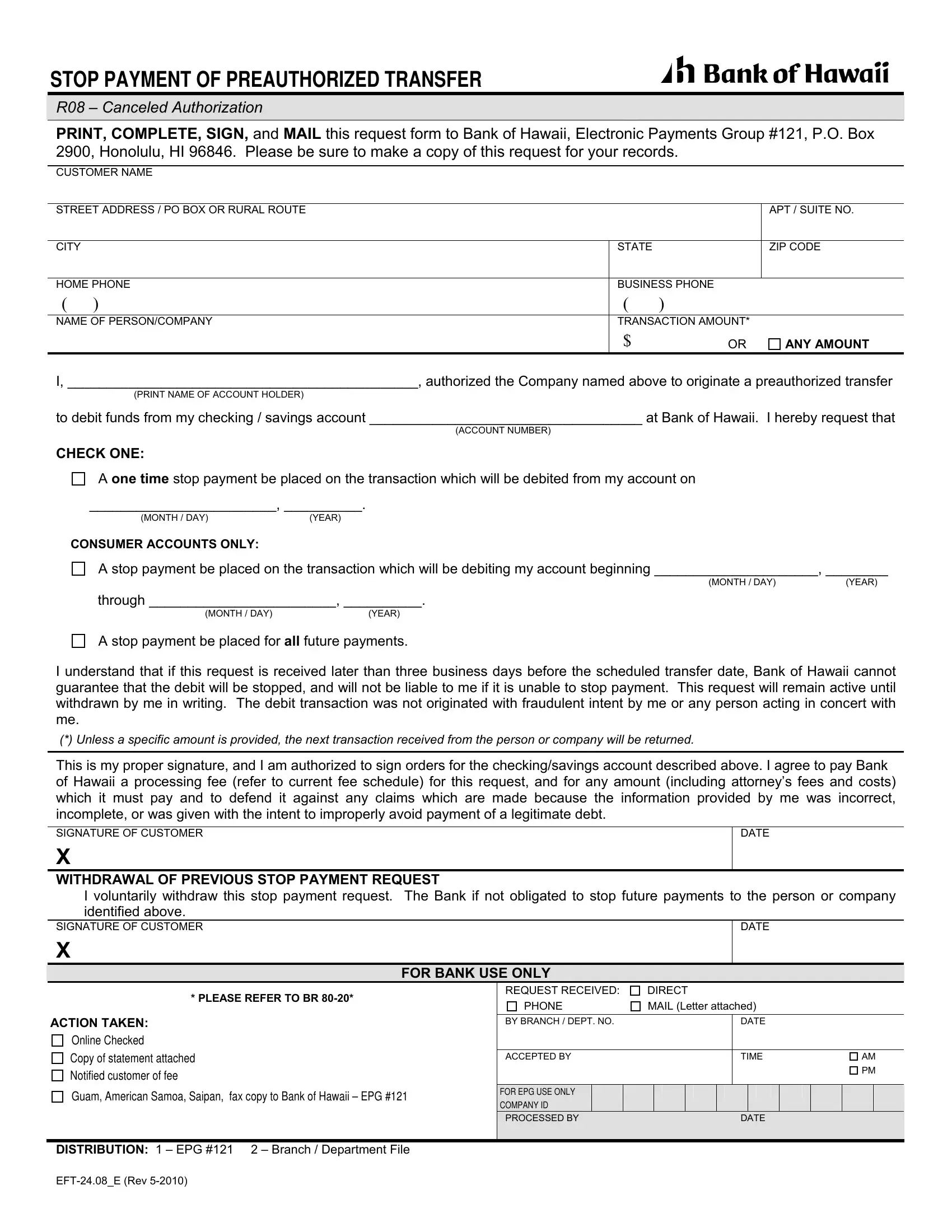
Managing your finances often involves keeping track of numerous transactions, especially automated ones. For situations where you need to stop a preauthorized transfer from your account, the EFT 24 08 E form provided by Bank of Hawaii offers a clear process. This form caters to customers who have previously authorized a company to debit their checking or savings account but now wish to halt these transactions. It allows for various options: putting a halt on a single upcoming transaction, stopping all transactions within a specified range, or ceasing all future payments to the specified recipient. To ensure effectiveness, the form must be submitted in a timely manner, specifically three business days before the scheduled transfer date. Furthermore, if the stop request is due to an unauthorized transaction, this form stands as a declaration that such transaction was not initiated with any fraudulent intent by the account holder. Alongside its primary function, the form also includes a section for withdrawing a previous stop payment request, offering flexibility to adjust decisions as financial situations change. Completing, signing, and mailing this form back to the Bank of Hawaii's specified address, while bearing in mind any processing fees as outlined in the bank’s fee schedule, embodies a simple yet crucial step for individuals aiming to manage their financial transactions more effectively.
| Question | Answer |
|---|---|
| Form Name | Form Eft 24 08 E |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | EFT 24.08_E bank of hawaii stop payment form |
STOP PAYMENT OF PREAUTHORIZED TRANSFER
R08 – Canceled Authorization
PRINT, COMPLETE, SIGN, and MAIL this request form to Bank of Hawaii, Electronic Payments Group #121, P.O. Box 2900, Honolulu, HI 96846. Please be sure to make a copy of this request for your records.
CUSTOMER NAME
STREET ADDRESS / PO BOX OR RURAL ROUTE |
|
|
APT / SUITE NO. |
|
|
|
|
|
|
CITY |
|
STATE |
|
ZIP CODE |
|
|
|
||
HOME PHONE |
BUSINESS PHONE |
|
||
( |
) |
( |
) |
|
|
|
|
||
NAME OF PERSON/COMPANY |
TRANSACTION AMOUNT* |
|
||
|
|
$ |
OR |
ANY AMOUNT |
I, _____________________________________________, authorized the Company named above to originate a preauthorized transfer
(PRINT NAME OF ACCOUNT HOLDER)
to debit funds from my checking / savings account ___________________________________ at Bank of Hawaii. I hereby request that
(ACCOUNT NUMBER)
CHECK ONE:
A ONE TIME stop payment be placed on the transaction which will be debited from my account on
________________________, __________.
(MONTH / DAY)(YEAR)
CONSUMER ACCOUNTS ONLY:
A stop payment be placed on the transaction which will be debiting my account beginning _____________________, ________
(MONTH / DAY)(YEAR)
through ________________________, __________.
(MONTH / DAY) |
(YEAR) |
A stop payment be placed for ALL future payments.
I understand that if this request is received later than three business days before the scheduled transfer date, Bank of Hawaii cannot guarantee that the debit will be stopped, and will not be liable to me if it is unable to stop payment. This request will remain active until withdrawn by me in writing. The debit transaction was not originated with fraudulent intent by me or any person acting in concert with me.
(*) Unless a specific amount is provided, the next transaction received from the person or company will be returned.
This is my proper signature, and I am authorized to sign orders for the checking/savings account described above. I agree to pay Bank of Hawaii a processing fee (refer to current fee schedule) for this request, and for any amount (including attorney’s fees and costs) which it must pay and to defend it against any claims which are made because the information provided by me was incorrect, incomplete, or was given with the intent to improperly avoid payment of a legitimate debt.
SIGNATURE OF CUSTOMER
X
DATE
WITHDRAWAL OF PREVIOUS STOP PAYMENT REQUEST
I voluntarily withdraw this stop payment request. The Bank if not obligated to stop future payments to the person or company identified above.
SIGNATURE OF CUSTOMER
X
DATE
FOR BANK USE ONLY
* PLEASE REFER TO BR |
|
REQUEST RECEIVED: |
|
DIRECT |
|
|
|
|
||||||||
|
PHONE |
|
MAIL (Letter attached) |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|||||||||
ACTION TAKEN: |
|
|
BY BRANCH / DEPT. NO. |
|
|
|
|
|
DATE |
|
|
|
|
|||
Online Checked |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Copy of statement attached |
|
|
ACCEPTED BY |
|
|
|
|
|
TIME |
|
|
AM |
||||
Notified customer of fee |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Guam, American Samoa, Saipan, fax copy to Bank of Hawaii – EPG #121 |
FOR EPG USE ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
COMPANY ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
PROCESSED BY |
|
|
|
|
|
DATE |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISTRIBUTION: 1 – EPG #121 |
2 – Branch / Department File |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|