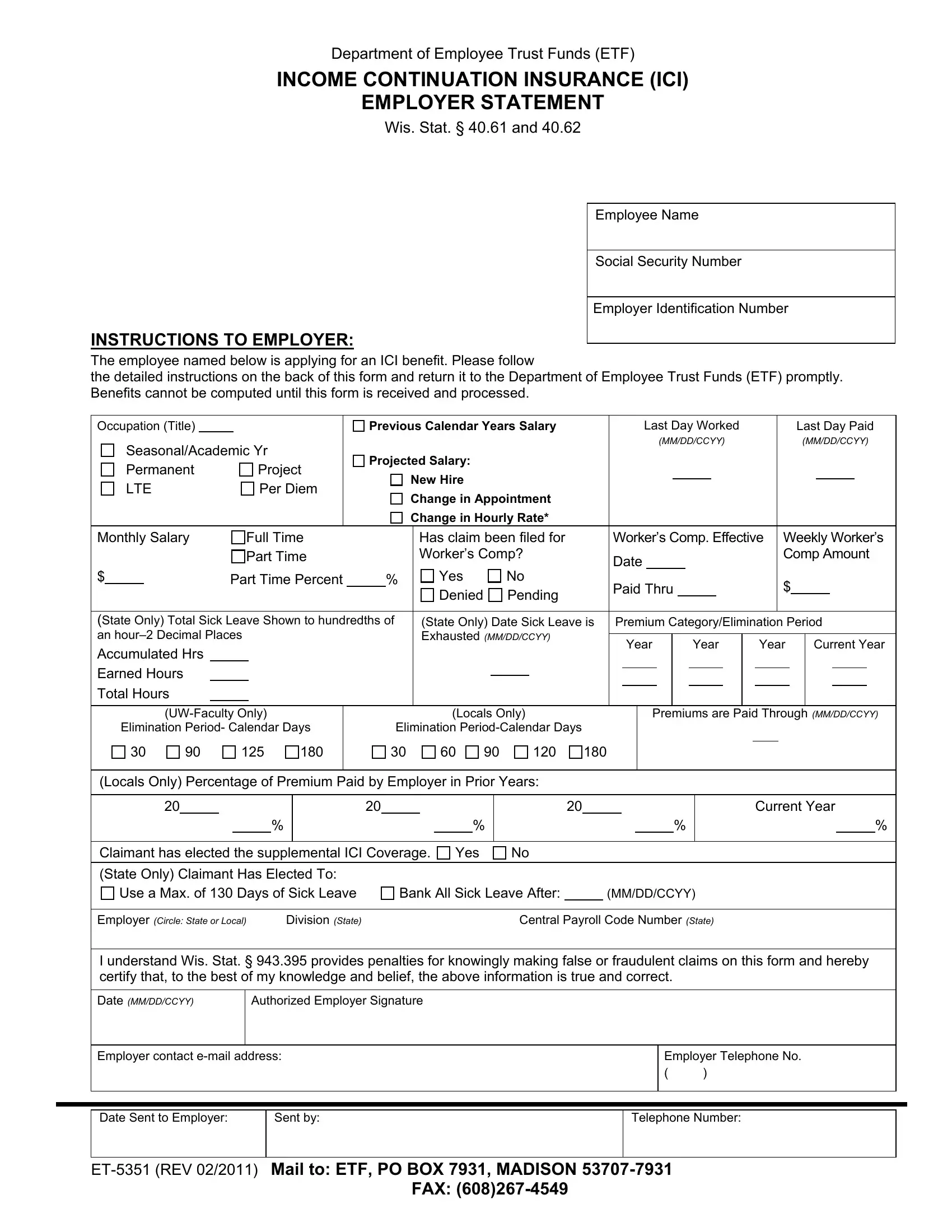
The ET-5351 form, a crucial document managed by the Department of Employee Trust Funds (ETF), possesses significant importance for both employers and employees within the context of Income Continuation Insurance (ICI) claims. This form serves a dual purpose: it not only facilitates the application process for employees seeking ICI benefits but also ensures that employers provide essential employment and salary details to the ETF. Specific elements such as the employee's name, social security number, occupation, salary details, and the nature of their employment status are meticulously captured to assess eligibility and compute benefits accurately. Furthermore, the form addresses various scenarios, including changes in appointment, salary adjustments, and eligibility for worker's compensation, which can influence the calculation of ICI benefits. Employers are also instructed to report sick leave accruals, premium payments, and any elected supplemental ICI coverage, thereby offering a comprehensive view of the employee's situation. By meticulously adhering to the instructions and submitting accurate information, employers play a pivotal role in ensuring their employees can access the financial support offered by ICI benefits during times of need.
| Question | Answer |
|---|---|
| Form Name | Form Et 5351 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | et5351 wt7 form |
