
Making use of the online tool for PDF editing by FormsPal, it is easy to fill in or edit Form F 01159 here and now. To make our editor better and less complicated to use, we consistently work on new features, taking into account suggestions from our users. This is what you'd want to do to get going:
Step 1: Press the orange "Get Form" button above. It is going to open our pdf tool so you could start filling in your form.
Step 2: Once you access the editor, there'll be the document prepared to be filled out. Aside from filling in various blank fields, you may also perform other things with the PDF, specifically adding any textual content, changing the original text, adding images, placing your signature to the document, and more.
In order to finalize this form, make certain you type in the necessary information in every area:
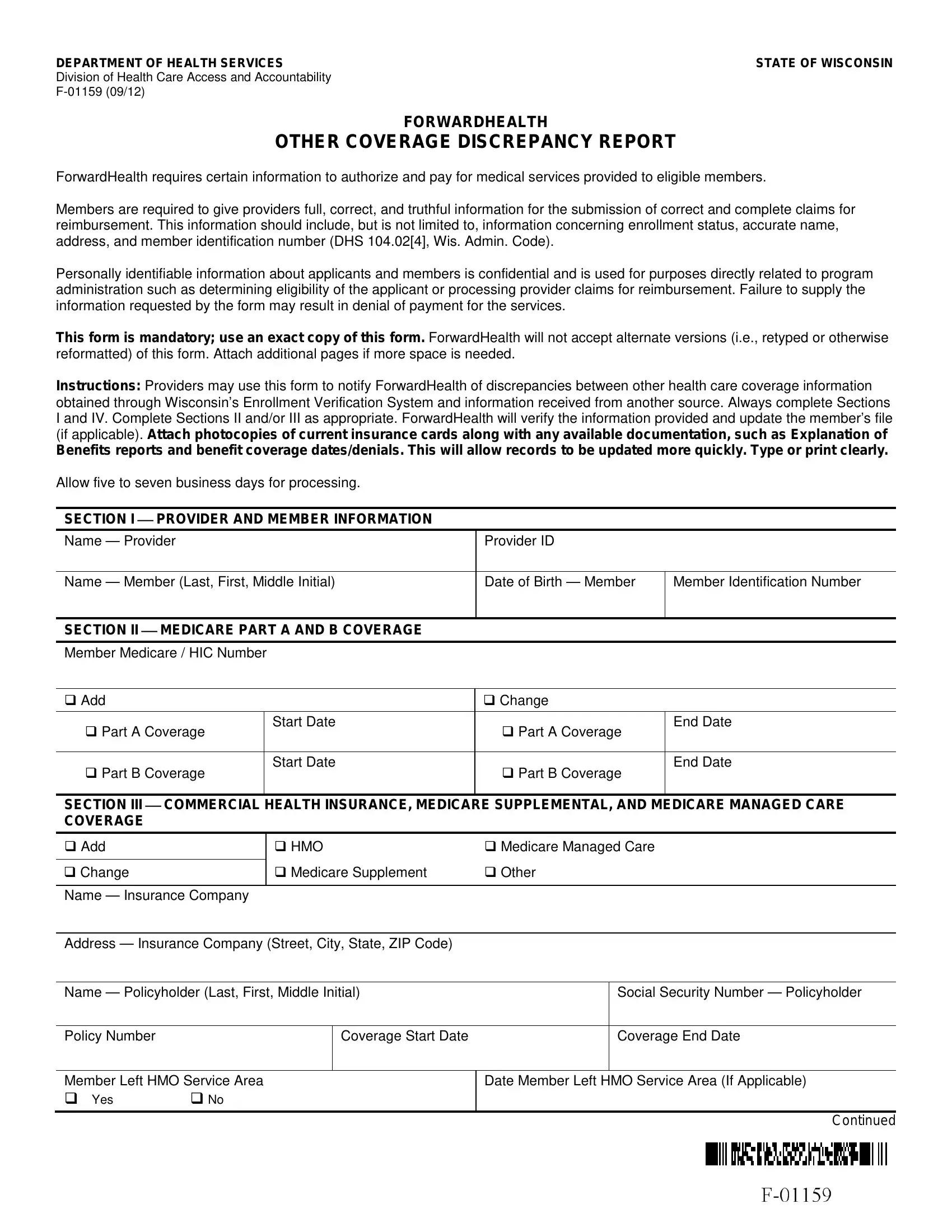
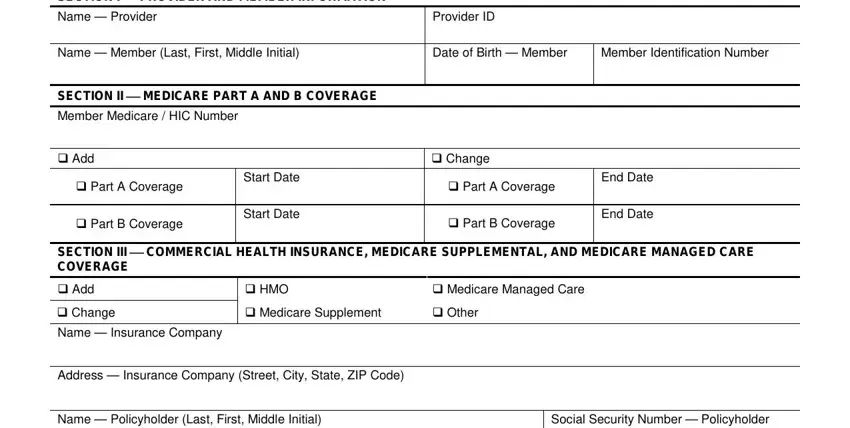
1. First, once filling out the Form F 01159, start in the form section with the next blank fields:
2. Right after this part is completed, go to type in the applicable information in all these - Policy Number, Coverage Start Date, Coverage End Date, Member Left HMO Service Area Yes, Date Member Left HMO Service Area, and Continued.
Always be very careful while filling out Coverage Start Date and Date Member Left HMO Service Area, because this is the section in which most users make a few mistakes.
3. Completing SECTION IV REPORT INFORMATION, Date Signed, Telephone Number Extension, Name Source of Information, Telephone Number Extension, Mail to, ForwardHealth Coordination of, Fax to, Coordination of Benefits, Comments, and Attach copy of insurance card is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Step 3: Right after double-checking the entries, press "Done" and you're done and dusted! Sign up with us now and immediately use Form F 01159, ready for downloading. Every last edit made is handily preserved , which means you can edit the form later on if required. Here at FormsPal, we do our utmost to be sure that all of your details are stored secure.