Understanding the intricacies and impact of the F-10106 form issued by the State of Wisconsin Department of Health Services is crucial for Wisconsin residents navigating the Medicare and Medicaid landscape. This form is a lifeline for Qualified Medicare Beneficiary (QMB), Specified Low-Income Medicare Beneficiary (SLMB), and SLMB+ recipients, marking the approval decision for Medicaid to cover certain Medicare expenses. For QMB participants, it entails Medicaid handling the costs associated with Medicare Part A and B premiums alongside cost-sharing obligations such as coinsurance, co-payments, and deductibles. SLMB and SLMB+ candidates see Medicaid covering their Part B premiums, though other Medicare-associated expenses remain their responsibility. The transition of billing Medicare premiums to Medicaid takes about two months, during which beneficiaries are encouraged to continue premium payments until notified of the switch. Moreover, the form outlines the right to appeal the eligibility determination, providing detailed steps and resources for initiating a fair hearing, along with the financial parameters used to assess eligibility. This form, therefore, is not just a notification—it is a comprehensive guide that informs beneficiaries about the specifics of their coverage, their rights to contest decisions, and the procedural steps for ensuring their Medicare and Medicaid benefits reflect their current financial and health status.
| Question | Answer |
|---|---|
| Form Name | Form F 10106 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | BADGERCARE, QMB, WISCONSIN, Unearned |
STATE OF WISCONSIN
DEPARTMENT OF HEALTH SERVICES
Division of Health Care Access and Accountability
Medicaid Qualified Medicare Beneficiary (QMB) / Specified
NOD
Recipient Name (Last, First, MI)
Case Number
Residence Address (Street, City, State, Zip Code)
Date
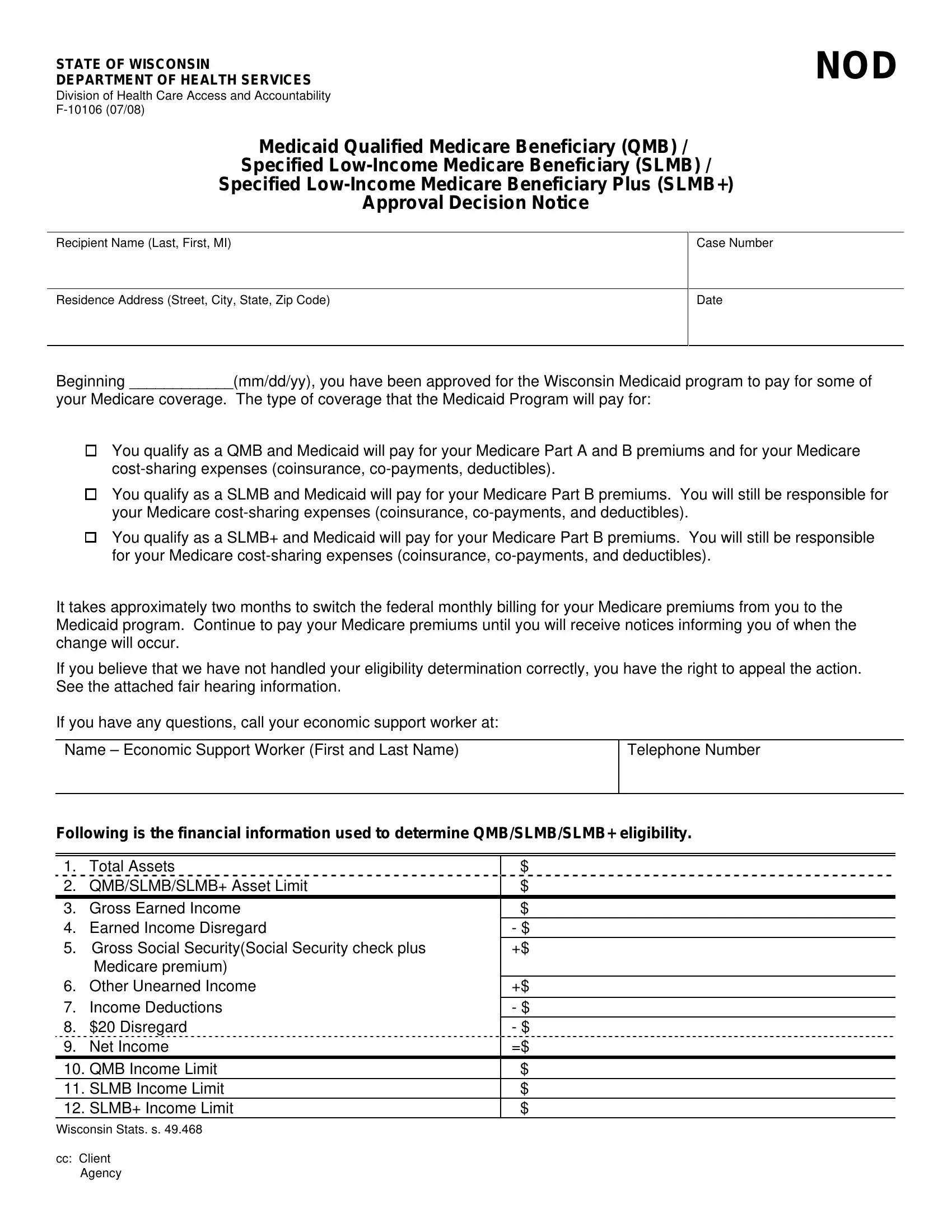
Beginning ____________(mm/dd/yy), you have been approved for the Wisconsin Medicaid program to pay for some of
your Medicare coverage. The type of coverage that the Medicaid Program will pay for:
¸ You qualify as a QMB and Medicaid will pay for your Medicare Part A and B premiums and for your Medicare
¸ You qualify as a SLMB and Medicaid will pay for your Medicare Part B premiums. You will still be responsible for your Medicare
¸ You qualify as a SLMB+ and Medicaid will pay for your Medicare Part B premiums. You will still be responsible for your Medicare
It takes approximately two months to switch the federal monthly billing for your Medicare premiums from you to the Medicaid program. Continue to pay your Medicare premiums until you will receive notices informing you of when the change will occur.
If you believe that we have not handled your eligibility determination correctly, you have the right to appeal the action. See the attached fair hearing information.
If you have any questions, call your economic support worker at:
Name – Economic Support Worker (First and Last Name) |
Telephone Number |
|
|
Following is the financial information used to determine QMB/SLMB/SLMB+ eligibility.
1. |
Total Assets |
$ |
|
|
|
|
|
|
|
|
|
|
2. |
QMB/SLMB/SLMB+ Asset Limit |
$ |
|
|
|
|
|
|
|
|
|
|
3. |
Gross Earned Income |
$ |
|
|
|
|
|
|
|
|
|
|
4. |
Earned Income Disregard |
- $ |
|
|
|
|
|
|
|
|
|
|
5. |
Gross Social Security(Social Security check plus |
+$ |
|
|
|
|
|
|
|
|
|
|
|
Medicare premium) |
|
|
|
|
|
|
|
|
|
|
|
6. |
Other Unearned Income |
+$ |
|
|
|
|
|
|
|
|
|
|
7. |
Income Deductions |
- $ |
|
|
|
|
|
|
|
|
|
|
8. |
$20 Disregard |
- $ |
|
|
|
|
|
|
|
|
|
|
9. |
Net Income |
=$ |
|
|
|
|
|
|
|
|
|
|
10. |
QMB Income Limit |
$ |
|
|
|
|
|
|
|
|
|
|
11. |
SLMB Income Limit |
$ |
|
|
|
|
|
|
|
|
|
|
12. |
SLMB+ Income Limit |
$ |
|
|
|
|
|
|
|
|
|
|
Wisconsin Stats. s. 49.468
cc:Client Agency
MEDICAID/BADGERCARE FAIR HEARING INFORMATION
If you are not satisfied with a Medicaid/BadgerCare decision you may appeal the decision by requesting a Fair Hearing in writing or in person at your local county/tribal social or human services department. You may also write to:
The Department of Administration
Division of Hearings and Appeals
PO Box 7875
Madison, WI
(608)
(608)
If you need an accommodation for a disability or a language translation, please call (608)
You, your chosen representative (if any), and the local county/tribal social or human services department will receive written notice at least 10 days before the fair hearing explaining the schedule time, date and place of the hearing. The hearing will be held in the county where you live.
If you file an appeal of a discontinuation, termination, or reduction of benefits before the date the change was to take effect, your coverage can continue pending the hearing decision. The appeal should include important facts of the matter and your Medicaid ID number.
Your request must be received within 45 days of the action you are appealing.
PREPARING FOR A FAIR HEARING
You have the right to bring witnesses, your own lawyer, or some other advisor to the fair hearing. The agency cannot pay for a lawyer to represent your side of the story, but they may be able to help you find free legal assistance for questions or fair hearing representation.
You have the right, both before the hearing and during the hearing, to see the agency’s written materials about the case, including your case record, upon which the agency based its decision.
You or your representative has the right to question anyone who testifies against you at the fair hearing. You also have the right to your own arguments and bring written materials showing why you think you are right.
If the fair hearing is about whether you are or are not incapacitated or disabled, you have the right to present medical evidence for proof, paid for by the agency.
If you cannot speak English or require sign language, you have the right to have an interpreter present at the hearing. The Division of Hearings and Appeals may authorize payment for necessary translation or interpreters if you ask.
CONTINUATION OF BENEFITS
If you ask for a fair hearing before the effective date of the agency’s action your Medicaid benefits will not be reduced or terminated until after the results of the fair hearing are known. You are still required to report any changes in your circumstances while your hearing is pending which may affect the level of your benefits. Asking for a fair hearing does not cancel out normally scheduled interview periods.
EFFECTS OF THE FAIR HEARING
If the fair hearing decision is in your favor:
̌No action will be taken against you by the agency.
̌If benefits have been terminated, they will be reinstated.
̌The date of reinstatement will be listed in the copy of the decision you receive, ordering the agency to reinstate your benefits.
If the fair hearing goes against you:
̌The agency’s action will stand and you may have to pay back the cost of any benefits you received that you should not have received.
REHEARINGS
After you have received the fair hearing decision, you have the right to ask for a rehearing if:
̌You have important new evidence that you could not have made available even if you tried, before the hearing that could change the decision.
̌You feel that there was a mistake in the facts of the decision.
̌You feel that there was a mistake in the legal basis of the decision.
If you would like a rehearing, a written request must be received within 20 days from the date of the written decision the Division of Hearings and Appeals. The state hearing’s office will decide within 30 days in a rehearing is justified.
APPEALING A FAIR HEARING OR REHEARING DECISION
If you do not agree with the fair hearing or rehearing decision, it is still possible for you to appeal to the Circuit Court in your county. This must be done within 30 days after you have received the written decision about the fair hearing or within 30 days of the denial of the rehearing request. An appeal to the Circuit Court must be completed by filing a petition with the Clerk of Courts in your county. It is best to have legal assistance, if you decide to appeal a fair hearing decision in Circuit Court.