
With the online editor for PDFs by FormsPal, you can easily fill out or edit Form F 10111 here. To make our tool better and more convenient to utilize, we constantly develop new features, with our users' suggestions in mind. All it takes is a few easy steps:
Step 1: Just press the "Get Form Button" in the top section of this site to get into our pdf form editing tool. Here you'll find all that is required to fill out your document.
Step 2: The editor will let you modify the majority of PDF forms in many different ways. Modify it with your own text, adjust what's originally in the document, and put in a signature - all when it's needed!
Concentrate while completing this form. Ensure all required fields are completed accurately.
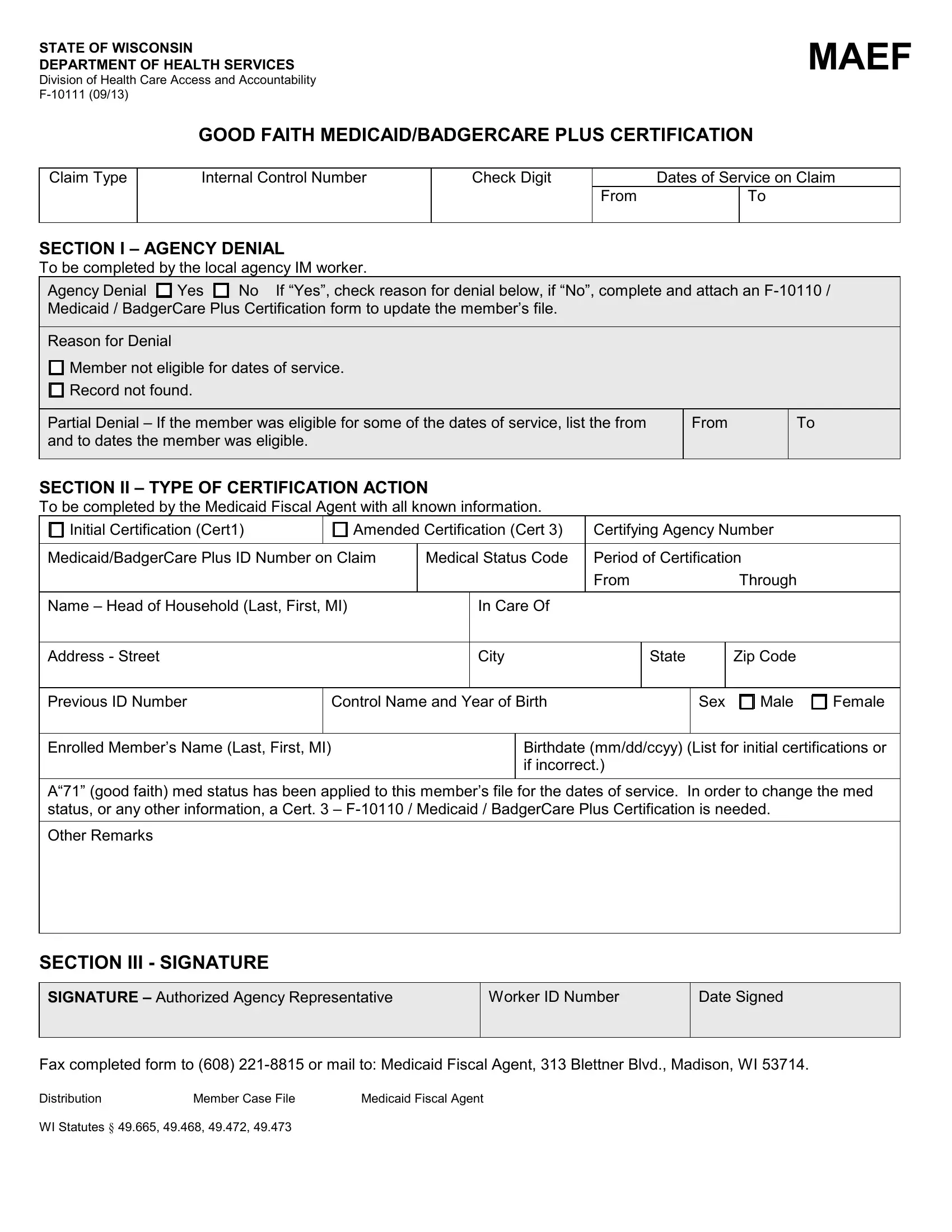
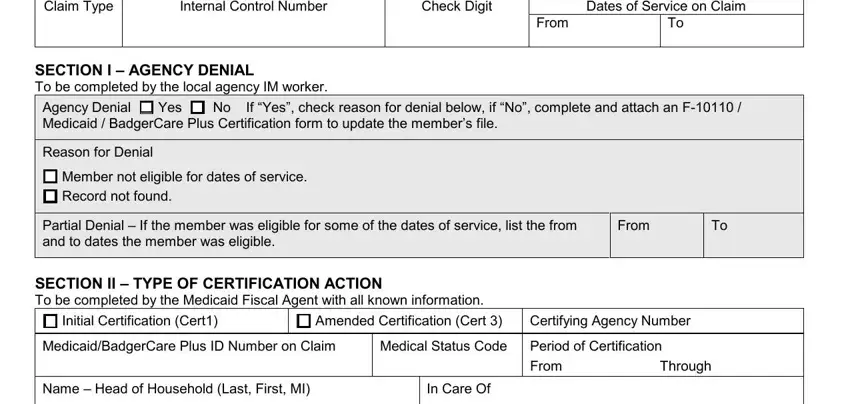
1. The Form F 10111 needs particular details to be inserted. Make certain the subsequent fields are finalized:
2. Right after filling in the last part, go on to the subsequent step and complete all required particulars in all these fields - Address Street, City, State, Zip Code, Previous ID Number, Control Name and Year of Birth, Sex, Male, Female, Enrolled Members Name Last First MI, A good faith med status has been, Birthdate mmddccyy List for, Other Remarks, SECTION III SIGNATURE, and SIGNATURE Authorized Agency.
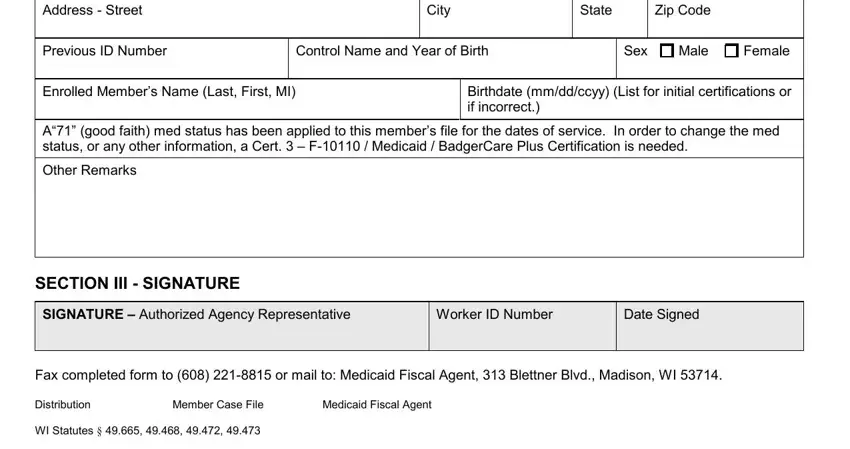
Be extremely careful when filling out Previous ID Number and Address Street, since this is where a lot of people make errors.
Step 3: Confirm that the information is accurate and click on "Done" to proceed further. Sign up with FormsPal right now and instantly get access to Form F 10111, ready for download. All alterations made by you are preserved , letting you modify the document later when necessary. Here at FormsPal, we aim to guarantee that all your information is kept private.