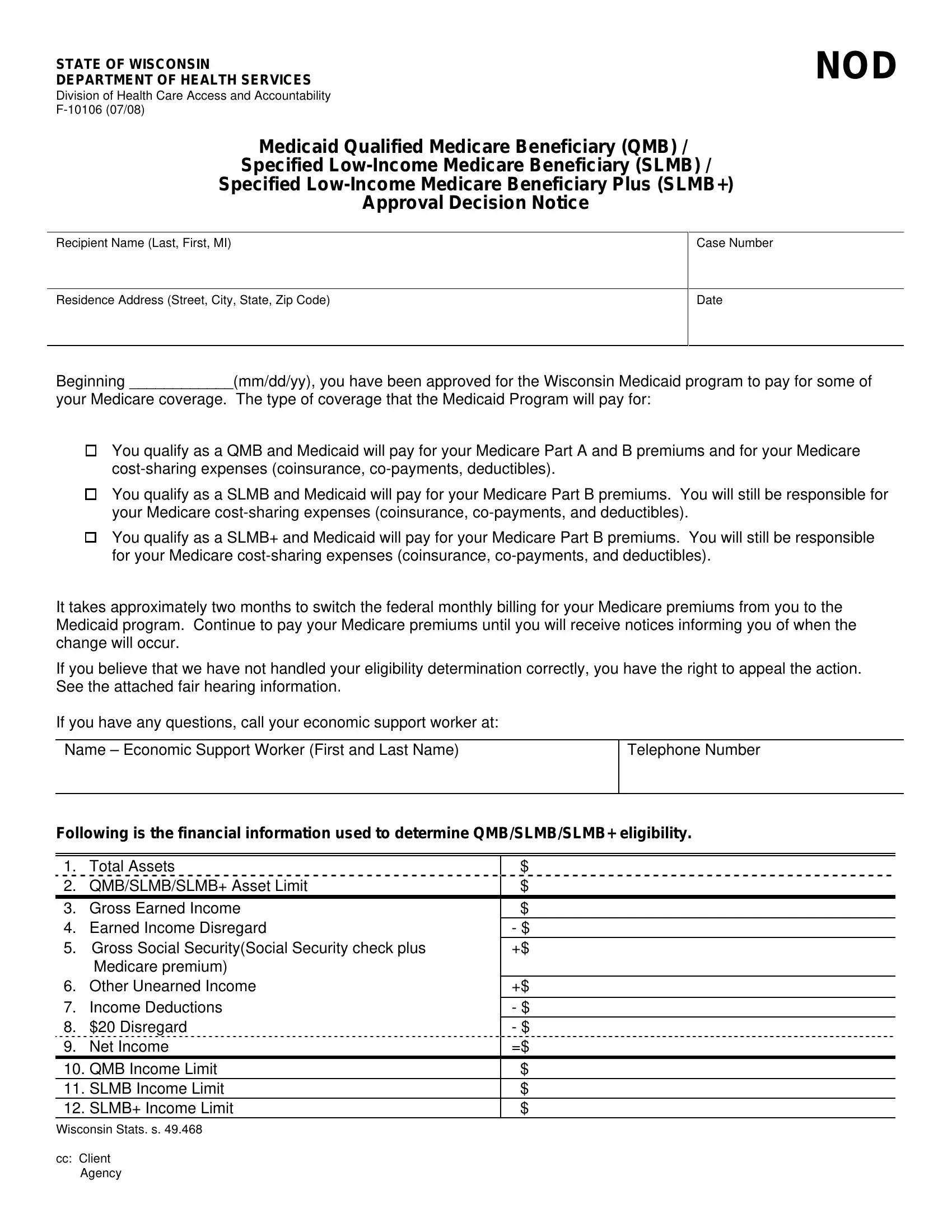
Understanding the intricacies and impact of the F-10106 form issued by the State of Wisconsin Department of Health Services is crucial for Wisconsin residents navigating the Medicare and Medicaid landscape. This form is a lifeline for Qualified Medicare Beneficiary (QMB), Specified Low-Income Medicare Beneficiary (SLMB), and SLMB+ recipients, marking the approval decision for Medicaid to cover certain Medicare expenses. For QMB participants, it entails Medicaid handling the costs associated with Medicare Part A and B premiums alongside cost-sharing obligations such as coinsurance, co-payments, and deductibles. SLMB and SLMB+ candidates see Medicaid covering their Part B premiums, though other Medicare-associated expenses remain their responsibility. The transition of billing Medicare premiums to Medicaid takes about two months, during which beneficiaries are encouraged to continue premium payments until notified of the switch. Moreover, the form outlines the right to appeal the eligibility determination, providing detailed steps and resources for initiating a fair hearing, along with the financial parameters used to assess eligibility. This form, therefore, is not just a notification—it is a comprehensive guide that informs beneficiaries about the specifics of their coverage, their rights to contest decisions, and the procedural steps for ensuring their Medicare and Medicaid benefits reflect their current financial and health status.
| Question | Answer |
|---|---|
| Form Name | Form F 10106 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | BADGERCARE, QMB, WISCONSIN, Unearned |
