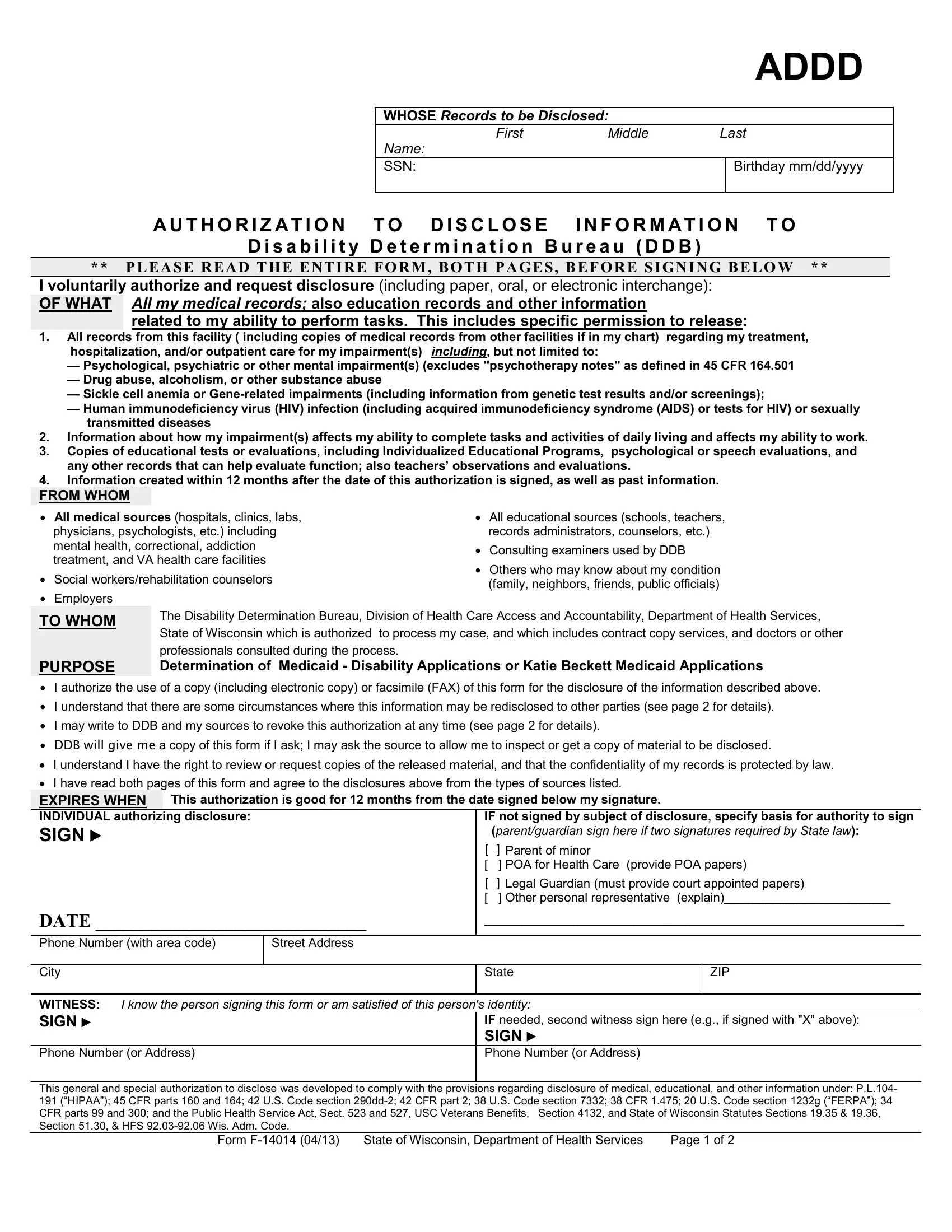
The Form F-14014, an essential document for individuals seeking Medicaid Disability or Katie Beckett Medicaid Applications within the State of Wisconsin, functions as a critical tool in the application process. This document, comprehensively designed, facilitates the authorized disclosure of a broad spectrum of personal information, ranging from medical, educational, to other pertinent details relevant to an applicant's disability assessment. By signing this form, an individual voluntarily agrees to the release of their records--including but not limited to medical histories, psychiatric evaluations, and educational assessments--to the Disability Determination Bureau (DDB). This process not only adheres to a plethora of legislative requirements, including HIPAA (Health Insurance Portability and Accountability Act) and FERPA (Family Educational Rights and Privacy Act) but also assures the confidentiality and protection of the individual's information under the Federal Privacy Act. The form intricately details the types of records that can be disclosed, specifies the recipients of such information, and underscores the purpose behind these disclosures, aiming to streamline the determination of eligibility for benefits while safeguarding applicants' privacy rights. Furthermore, it highlights the option for individuals to revoke this authorization, outlining the potential consequences of such actions on the processing of their claims. Offering a 12-month validity period from the date of signature, the Form F-14014 embodies a balance between the necessity of information sharing for disability determination and the imperative of protecting personal information in adherence to federal and state laws.
| Question | Answer |
|---|---|
| Form Name | Form F 14014 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | F14014 wi dhs authorization disclose form |
|
|
|
|
|
ADDD |
|
|
|
|
|
|
|
|
WHOSE Records to be Disclosed: |
|
|
|
|
|
First |
Middle |
Last |
|
|
|
Name: |
|
|
|
|
|
SSN: |
|
|
Birthday mm/dd/yyyy |
|
|
|
|
||
AU THO RI Z ATI O N TO DI SCLOS E |
INFO RMATI O N TO |
||||
Di sa bi li ty De te rmi na tion Bureau (DDB)
** PLEASE READ THE ENTIRE FORM, BOTH PAGES, BEFORE SIGNING BELOW **
I voluntarily authorize and request disclosure (including paper, oral, or electronic interchange):
OF WHAT All my medical records; also education records and other information
related to my ability to perform tasks. This includes specific permission to release:
1.All records from this facility ( including copies of medical records from other facilities if in my chart) regarding my treatment,
hospitalization, and/or outpatient care for my impairment(s) including, but not limited to:
—Psychological, psychiatric or other mental impairment(s) (excludes "psychotherapy notes" as defined in 45 CFR 164.501
—Drug abuse, alcoholism, or other substance abuse
—Sickle cell anemia or
—Human immunodeficiency virus (HIV) infection (including acquired immunodeficiency syndrome (AIDS) or tests for HIV) or sexually transmitted diseases
2.Information about how my impairment(s) affects my ability to complete tasks and activities of daily living and affects my ability to work.
3.Copies of educational tests or evaluations, including Individualized Educational Programs, psychological or speech evaluations, and any other records that can help evaluate function; also teachers’ observations and evaluations.
4.Information created within 12 months after the date of this authorization is signed, as well as past information.
FROM WHOM
∙All medical sources (hospitals, clinics, labs, physicians, psychologists, etc.) including mental health, correctional, addiction treatment, and VA health care facilities
∙Social workers/rehabilitation counselors
∙Employers
∙All educational sources (schools, teachers, records administrators, counselors, etc.)
∙Consulting examiners used by DDB
∙Others who may know about my condition (family, neighbors, friends, public officials)
TO WHOM
PURPOSE
The Disability Determination Bureau, Division of Health Care Access and Accountability, Department of Health Services, State of Wisconsin which is authorized to process my case, and which includes contract copy services, and doctors or other professionals consulted during the process.
Determination of Medicaid - Disability Applications or Katie Beckett Medicaid Applications
∙I authorize the use of a copy (including electronic copy) or facsimile (FAX) of this form for the disclosure of the information described above.
∙I understand that there are some circumstances where this information may be redisclosed to other parties (see page 2 for details).
∙I may write to DDB and my sources to revoke this authorization at any time (see page 2 for details).
∙DDB will give me a copy of this form if I ask; I may ask the source to allow me to inspect or get a copy of material to be disclosed.
•I understand I have the right to review or request copies of the released material, and that the confidentiality of my records is protected by law.
•I have read both pages of this form and agree to the disclosures above from the types of sources listed.
EXPIRES WHEN This authorization is good for 12 months from the date signed below my signature.
INDIVIDUAL authorizing disclosure:
SIGN ►
DATE _____________________________
IF not signed by subject of disclosure, specify basis for authority to sign
|
(parent/guardian sign here if two signatures required by State law): |
[ |
] Parent of minor |
[ |
] POA for Health Care (provide POA papers) |
[ |
] Legal Guardian (must provide court appointed papers) |
[ |
] Other personal representative (explain)________________________ |
_____________________________________________
Phone Number (with area code) |
Street Address |
|
|
|
|
|
|
City |
|
State |
ZIP |
|
|
|
|
WITNESS: I know the person signing this form or am satisfied of this person's identity: |
|
||
SIGN ► |
|
IF needed, second witness sign here (e.g., if signed with "X" above): |
|
|
|
SIGN ► |
|
Phone Number (or Address) |
|
Phone Number (or Address) |
|
|
|
|
|
This general and special authorization to disclose was developed to comply with the provisions regarding disclosure of medical, educational, and other information under: P.L.104- 191 (“HIPAA”); 45 CFR parts 160 and 164; 42 U.S. Code section
Form |
State of Wisconsin, Department of Health Services |
Page 1 of 2 |
Explanation of Form
“Authorization to Disability Determination Bureau (DDB)”
We need your written authorization to get the information required to process your application for Medicaid Disability or Katie Beckett Medicaid. Laws and regulations require that sources of personal information have a signed authorization before releasing it to the Disability Determination Bureau (DDB). Also, laws require specific authorization for the release of information about certain conditions and from educational sources.
You can provide this authorization by signing a Form
You have the right to revoke this authorization at any time, except to the extent a source of information has already relied on it to take an action. To do so, make a written request to your county social or human services department, the Katie Beckett Program or directly to the Disability Determination Bureau (P.O. Box 7886, Madison, WI
IMPORTANT INFORMATION, INCLUDING NOTICE REQUIRED BY THE PRIVACY ACT
All personal information collected by the DDB is protected by the Federal Privacy Act of 1974. Once medical information is disclosed to the DDB, it is no longer protected by the Health Insurance Portability and Accountability Act (HIPAA) health information privacy provisions (45 CFR part 164). The DDB retains personal information in strict adherence to the retention schedules established and maintained in conjunction with the National Archives and Records Administration. At the end of a record’s useful life cycle, it is destroyed in accordance with the privacy provisions, as specified in 36 CFR part 1228.
The DDB will use the information obtained with this form to determine your eligibility for benefits, and your ability to manage any benefits received. This use usually includes review of the information by DDB staff in processing your case. In some cases, your information may also be reviewed by DDB staff that process your appeal of a decision, or by investigators to resolve allegations of fraud or abuse, and may be used in any related administrative, civil, or criminal proceedings.
Signing this form is voluntary, but failing to sign it, or revoking it before we receive necessary information, could prevent an accurate or timely decision on your claim, and could result in denial or loss of benefits. Although the information we obtain with this form is used for the purposes stated above and the information may be disclosed by the DDB without your consent if authorized by Federal laws such as the Privacy Act and the Social Security Act. For example, the DDB may disclose:
1.To enable a third party (e.g., consulting physicians) or other government agency to assist the DDB to establish rights to Social Security benefits and/or Medicaid coverage;
2.To comply with State and local laws requiring the release of information in situations of suspected child or elder abuse.;
3.We may also use the information you give us when we match records by computer. Matching programs compare our records with those of other Federal, state, or local government agencies. Many agencies may use matching programs to find or prove that a person qualifies for benefits paid by the government. The law allows us to do this even if you do not agree to it.
If You Need Assistance in Completing This Authorization or Have Questions
If you need assistance in completing this authorization or if you have questions about the authorization, please contact the Medicaid office where you filed your application.
Form
Page 2 of 2