Our top level developers worked hard to obtain the PDF editor we are now proud to deliver to you. The software will allow you to instantly complete Form F 20483 and can save precious time. You just have to comply with this specific guideline.
Step 1: To get started, choose the orange button "Get Form Now".
Step 2: It's now possible to modify your Form F 20483. Our multifunctional toolbar makes it possible to add, delete, adapt, and highlight content material or conduct other commands.
All of the following areas will make up your PDF file:
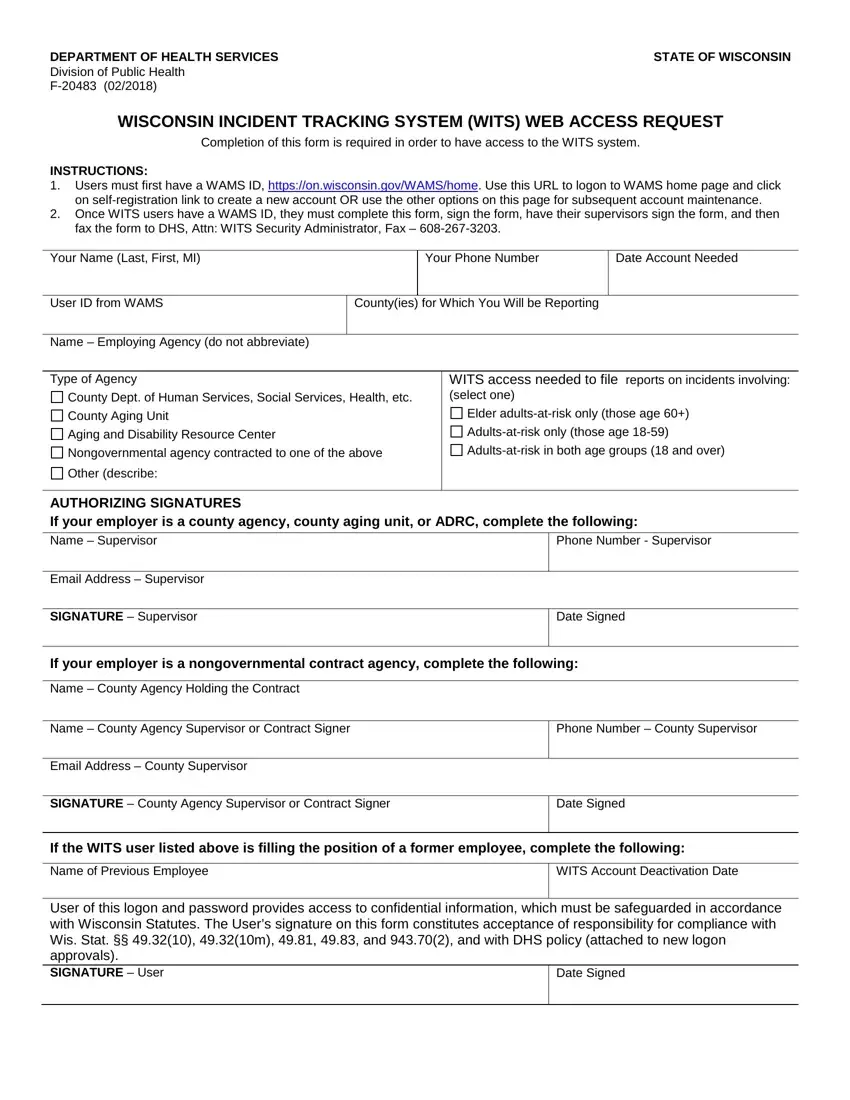
Complete the SIGNATURE Supervisor, Date Signed, If your employer is a, Name County Agency Holding the, Name County Agency Supervisor or, Phone Number County Supervisor, Email Address County Supervisor, SIGNATURE County Agency, Date Signed, If the WITS user listed above is, Name of Previous Employee, WITS Account Deactivation Date, User of this logon and password, and Date Signed field using the data requested by the software.
Step 3: Choose "Done". You can now export the PDF document.
Step 4: It can be more convenient to create copies of your document. You can rest assured that we won't display or check out your information.
