
Should you desire to fill out Form F212 233 Ooo, you don't have to download any applications - simply try our PDF tool. In order to make our tool better and easier to utilize, we consistently work on new features, bearing in mind suggestions from our users. Starting is simple! All you have to do is stick to the following simple steps below:
Step 1: Simply click the "Get Form Button" above on this page to start up our form editor. There you'll find everything that is necessary to work with your document.
Step 2: As soon as you launch the online editor, there'll be the form ready to be filled in. Apart from filling out different blank fields, it's also possible to perform various other things with the PDF, such as putting on custom textual content, modifying the original textual content, inserting illustrations or photos, putting your signature on the PDF, and more.
This document needs some specific information; to ensure correctness, please make sure to take note of the tips hereunder:
1. While submitting the Form F212 233 Ooo, be sure to complete all necessary blanks within the relevant section. This will help speed up the process, enabling your details to be handled fast and appropriately.
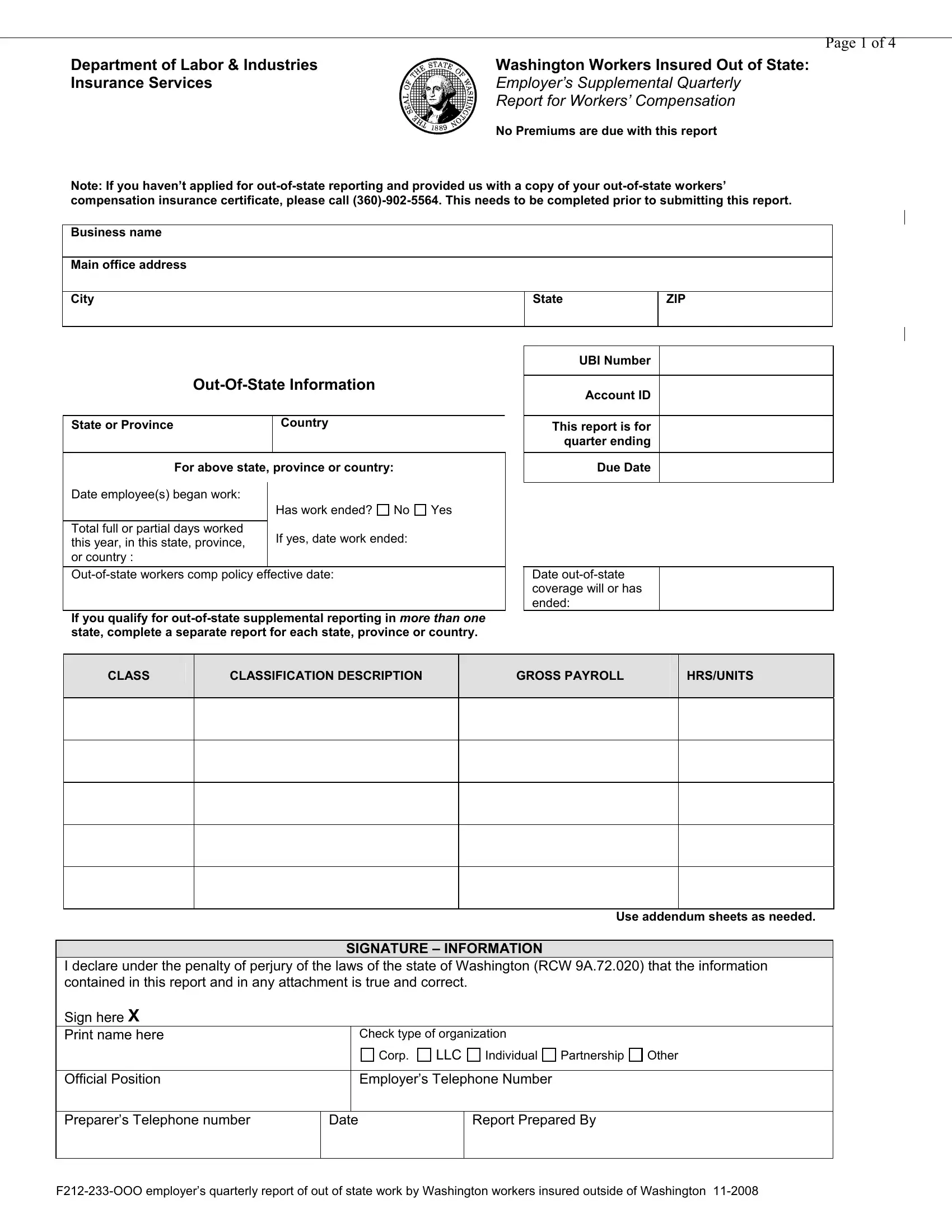
2. After filling in the previous step, go to the next part and fill out the necessary particulars in all these fields - CLASS, CLASSIFICATION DESCRIPTION, GROSS PAYROLL, HRSUNITS, Use addendum sheets as needed, SIGNATURE INFORMATION, I declare under the penalty of, Check type of organization, Individual, Partnership, Other, Corp, LLC, Official Position, and Employers Telephone Number.
3. The third stage will be hassle-free - complete all of the form fields in FIRST NAME, LAST NAME, and SOCIAL SECURITY NUMBER to conclude the current step.
4. Completing SEND TO THIS ADDRESS Dept of Labor, and Use addendum sheets as needed is crucial in the next section - don't forget to take the time and take a close look at every single blank area!
5. And finally, this last subsection is what you should wrap up before submitting the PDF. The blank fields in question are the following: Classification Addendum for, Business Name, OutOfState Information State or, Country, UBI Number, Account ID, This report is for Quarter Ending, CLASSIFICATION DESCRIPTION, GROSS PAYROLL, CLASS, and HRSUNITS.
People who use this document generally make mistakes when completing GROSS PAYROLL in this section. Be certain to reread whatever you type in right here.
Step 3: Glance through all the information you've inserted in the blanks and hit the "Done" button. Grab your Form F212 233 Ooo the instant you sign up at FormsPal for a 7-day free trial. Immediately gain access to the form from your personal cabinet, along with any edits and adjustments being conveniently synced! FormsPal guarantees your data confidentiality by having a secure system that in no way records or distributes any type of personal data used. Feel safe knowing your paperwork are kept protected when you work with our services!