
 Update Visit (annual)
Update Visit (annual)
 Significant Change in Condition
Significant Change in Condition
 Temporary Service Authorization
Temporary Service Authorization


 Information Only
Information Only
 Cancel Authorization
Cancel Authorization



 No Serious Occurrences
No Serious Occurrences
It won't be challenging to obtain FA-24 working with our PDF editor. Here's how you can easily easily design your file.
Step 1: Click on the button "Get Form Here".
Step 2: At the moment, it is possible to alter your FA-24. Our multifunctional toolbar makes it possible to include, delete, adapt, highlight, as well as undertake other commands to the words and phrases and fields within the form.
Provide the content demanded by the application to complete the file.
Note the necessary data in the field Recipient Ineligible Recipient, SECTION CONTACT INFORMATION, RECIPIENT INFORMATION, Last Name, Recipient Medicaid ID, Translator Required, Yes, First Name, Date of Birth, Language, Address, City, State, Zip Code, and Phone.
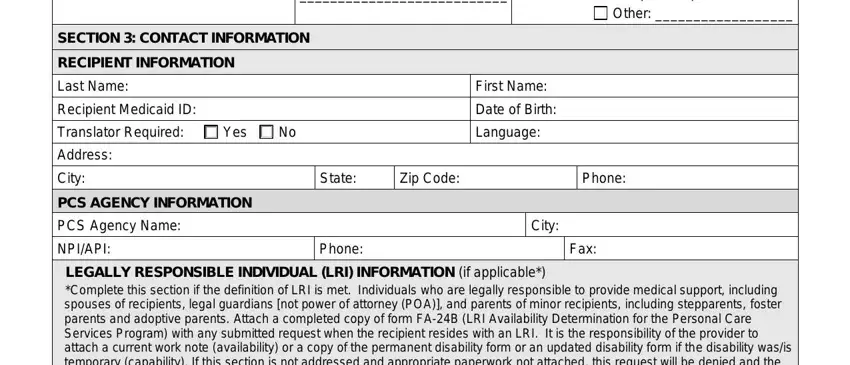
It's important to provide specific particulars within the space LEGALLY RESPONSIBLE INDIVIDUAL LRI, Does recipient have an LRI see, Yes, Unknown, LRI Name, Relationship to Recipient, Phone, Does LRI reside with recipient, Yes, Is the LRI also on the PCS Program, Yes, No Receives hrswk, LRI Employment Status, Employed Hrswk Days Off, and Unemployed.
The space Nevada Medicaid and Check Up, Recipient Name, Recipient Medicaid ID, ALTERNATE CONTACT INFORMATION An, Alternate Contact Name, Phone, Relationship to Recipient, Can this person be contacted in, Yes, SECTION DIAGNOSES AND INCIDENTS, DIAGNOSISDIAGNOSES AFFECTING THE, Is anyone else in the home, Yes Who, Unknown, and INCIDENTS INCLUDING A SUMMARY OF is where you include all parties' rights and responsibilities.
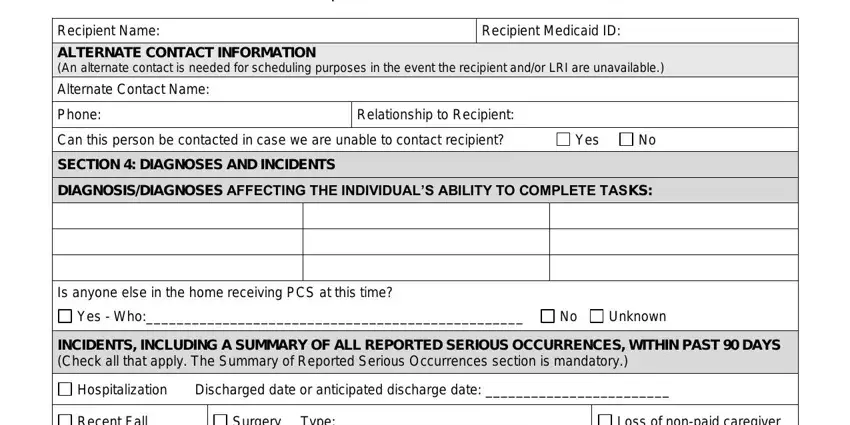
Finalize by reviewing these sections and filling them in as required: Recent Fall, Surgery, Type, Loss of nonpaid caregiver, New Medical ConditionDiagnosis, Addition or loss of other services, Summary of Reported Serious, No Serious Occurrences, and SECTION COMMENTS General comments.
Step 3: Click the Done button to save your document. Now it is at your disposal for export to your electronic device.
Step 4: It may be simpler to have duplicates of the file. You can rest easy that we are not going to display or see your particulars.
