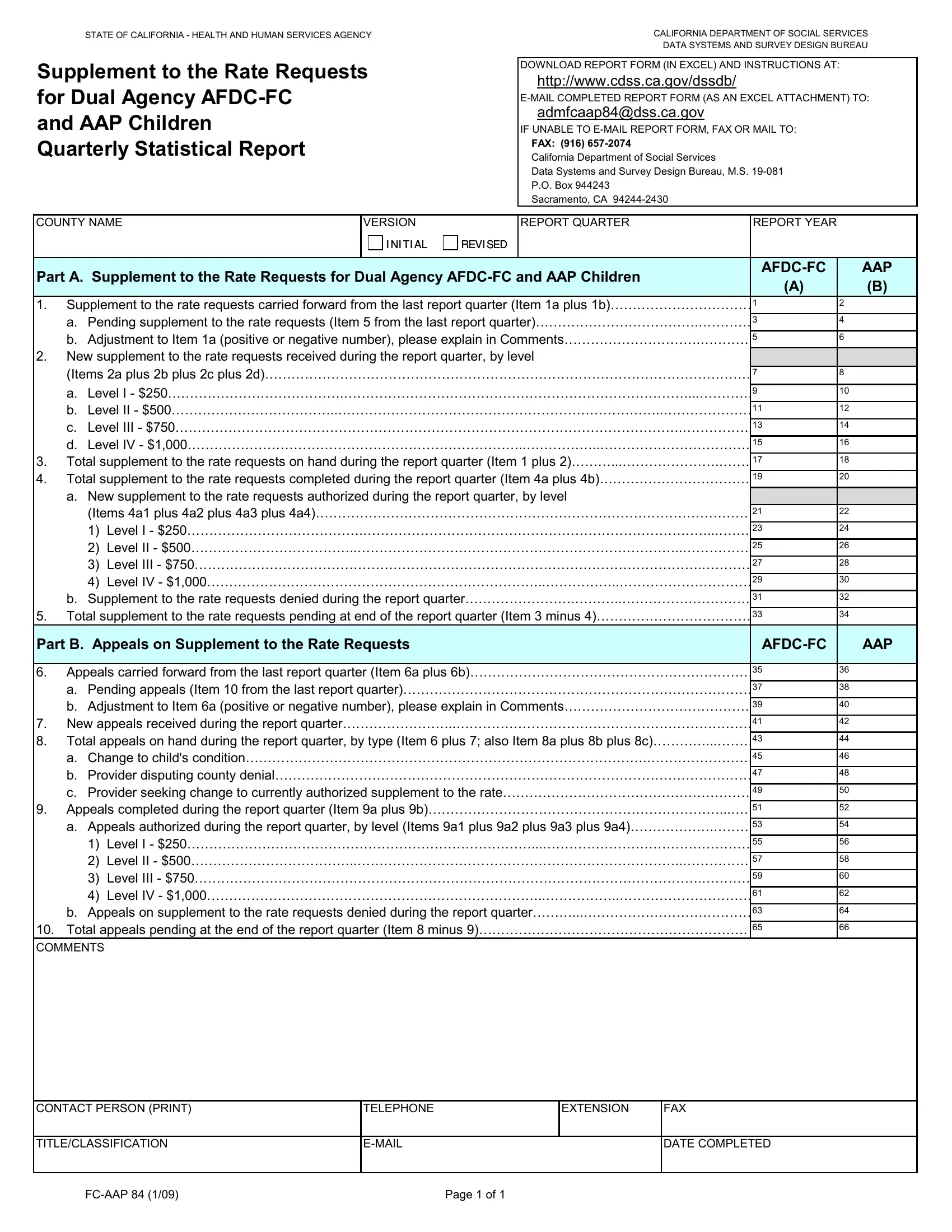
In the realm of child welfare and support within the State of California, the Fc Aap 84 form emerges as a crucial document detailing Supplement to the Rate Requests for Dual Agency AFDC-FC (Aid to Families with Dependent Children-Foster Care) and AAP (Adoption Assistance Program) Children on a quarterly basis. This comprehensive report, produced by the California Department of Social Services Data Systems and Survey Design Bureau, serves multiple fundamental purposes. It acts as a quantitative basis for adjustments and enhancements in the provisions for children under the dual agency care, encompassing those in foster care and those who have been adopted. Through precise statistical reporting, the form captures the genesis, adjustment, authorization, or denial of additional support rates, delineating them across different levels based on the necessity of care. Furthermore, it meticulously documents appeals concerning rate adjustments, thereby facilitating transparency and accountability in the assessment and support of children's needs. This structured mechanism not only assists in optimal resource allocation by county welfare departments but also underpins the legislative oversight on such matters, following the mandates set by SB 84. The accessibility of this form via download in Excel format from the department's website and its submission either electronically or through traditional mail/fax underscores the adaptability and efficiency intended in its design. The data elicited through this form are indispensable for budgeting, staffing, program planning, and strategic decision-making by county, state, and federal entities, highlighting its critical role in the broader context of social services delivery and policy formulation.
| Question | Answer |
|---|---|
| Form Name | Form Fc Aap 84 |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | E-MAIL, DDS, AAP, Lanterman |
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY
Supplement to the Rate Requests for Dual Agency
and AAP Children Quarterly Statistical Report
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES
DATA SYSTEMS AND SURVEY DESIGN BUREAU
DOWNLOAD REPORT FORM (IN EXCEL) AND INSTRUCTIONS AT:
http://www.cdss.ca.gov/dssdb/
admfcaap84@dss.ca.gov
IF UNABLE TO
FAX: (916)
California Department of Social Services
Data Systems and Survey Design Bureau, M.S.
P.O. Box 944243
Sacramento, CA
COUNTY NAME |
VERSION |
|
|
REPORT QUARTER |
REPORT YEAR |
|
|
||||
|
|
|
|
I NI TI AL |
|
REVI SED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Part A. Supplement to the Rate Requests for Dual Agency |
|
AAP |
|||||||||
|
(A) |
|
(B) |
||||||||
|
|
|
|
|
|
|
|
|
|
||
1. |
Supplement to the rate requests carried forward from the last report quarter (Item 1a plus 1b)…………………………… |
1 |
|
2 |
|
||||||
|
a. Pending supplement to the rate requests (Item 5 from the last report quarter)……………………………….………… |
3 |
|
4 |
|
||||||
|
b. Adjustment to Item 1a (positive or negative number), please explain in Comments………………………….………… |
5 |
|
6 |
|
||||||
2. |
New supplement to the rate requests received during the report quarter, by level |
|
|
|
|
||||||
|
(Items 2a plus 2b plus 2c plus 2d)………………………………………………………………………………………………… |
7 |
|
8 |
|
||||||
|
|
|
|
|
|
|
|
|
|||
|
a. Level I - $250………………………………….……………………………………………………………………...………… |
9 |
|
10 |
|
||||||
|
b. Level II - $500………………………………..………………………………………………………………..………………… |
11 |
|
12 |
|
||||||
|
c. Level III - $750…………………………………………………………………………………………………….…………… |
13 |
|
14 |
|
||||||
|
d. Level IV - $1,000…………………………………………………………………..……………..……………………………… |
15 |
|
16 |
|
||||||
3. |
Total supplement to the rate requests on hand during the report quarter (Item 1 plus 2)………...………………….……… |
17 |
|
18 |
|
||||||
4. |
Total supplement to the rate requests completed during the report quarter (Item 4a plus 4b)……………………………… |
19 |
|
20 |
|
||||||
|
a. New supplement to the rate requests authorized during the report quarter, by level |
|
|
|
|
||||||
|
(Items 4a1 plus 4a2 plus 4a3 plus 4a4)……………………………………………………………………………………… |
21 |
|
22 |
|
||||||
|
1) Level I - $250………………………………….……………………………………………………………………...……… |
23 |
|
24 |
|
||||||
|
2) Level II - $500………………………………..………………………………………………………………..…………… |
25 |
|
26 |
|
||||||
|
3) Level III - $750…………………………………………………………………………………………………….………… |
27 |
|
28 |
|
||||||
|
4) Level IV - $1,000…………………………………………………………………..……………..………………………… |
29 |
30 |
|
|||||||
|
b. Supplement to the rate requests denied during the report quarter…………………….………..………………………… |
31 |
|
32 |
|
||||||
5. |
Total supplement to the rate requests pending at end of the report quarter (Item 3 minus 4)……………………………… |
33 |
|
34 |
|
||||||
Part B. Appeals on Supplement to the Rate Requests |
|
|
|
|
AAP |
||||||
|
|
|
|
|
|
|
|
|
|||
6. |
Appeals carried forward from the last report quarter (Item 6a plus 6b)………………………………………………………… |
35 |
|
36 |
|
||||||
|
a. Pending appeals (Item 10 from the last report quarter)……………………………………………………………………… |
37 |
|
38 |
|
||||||
|
b. Adjustment to Item 6a (positive or negative number), please explain in Comments…………………………………… |
39 |
|
40 |
|
||||||
7. |
New appeals received during the report quarter……………………..…………………………………………………………… |
41 |
|
42 |
|
||||||
8. |
Total appeals on hand during the report quarter, by type (Item 6 plus 7; also Item 8a plus 8b plus 8c)…………...……… |
43 |
|
44 |
|
||||||
|
a. Change to child's condition……………………………………………………………………………….…………………… |
45 |
|
46 |
|
||||||
|
b. Provider disputing county denial……………………………………………………………………………………………… |
47 |
|
48 |
|
||||||
|
c. Provider seeking change to currently authorized supplement to the rate………………………………………………… |
49 |
|
50 |
|
||||||
9. |
Appeals completed during the report quarter (Item 9a plus 9b)…………………………………………………………...…… |
51 |
|
52 |
|
||||||
|
a. Appeals authorized during the report quarter, by level (Items 9a1 plus 9a2 plus 9a3 plus 9a4)……………….……… |
53 |
|
54 |
|
||||||
|
1) Level I - $250……………………………………………………………………...………………………………………… |
55 |
|
56 |
|
||||||
|
2) Level II - $500………………………………..………………………………………………………………..…………… |
57 |
|
58 |
|
||||||
|
3) Level III - $750…………………………………………………………………………………………………….………… |
59 |
|
60 |
|
||||||
|
4) Level IV - $1,000…………………………………………………………………..……………..………………………… |
61 |
|
62 |
|
||||||
|
b. Appeals on supplement to the rate requests denied during the report quarter………...………………………………… |
63 |
|
64 |
|
||||||
10. |
Total appeals pending at the end of the report quarter (Item 8 minus 9)……………………………………………………. |
65 |
|
66 |
|
||||||
COMMENTS
CONTACT PERSON (PRINT) |
TELEPHONE |
EXTENSION |
FAX |
|
|
|
|
TITLE/CLASSIFICATION |
|
DATE COMPLETED |
|
|
|
|
|
Page 1 of 1 |
STATE OF CALIFORNIA – HEALTH AND HUMAN SERVICES AGENCY |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
|
DATA SYSTEMS AND SURVEY DESIGN BUREAU |
SUPPLEMENT TO THE RATE REQUESTS FOR DUAL AGENCY
INSTRUCTIONS
CONTENT
The Supplement to the Rate Requests for Dual Agency Aid to Families with Dependent
PURPOSE
In 2007, the California Legislature passed SB 84 (Chapter 177, Statutes of 2007), which requires the CDSS and the Department of Developmental Services (DDS) to report semiannually to the Legislature data collected on the number and nature of supplement to the rate requests. The supplement to the rate is established by Welfare & Institutions Code (W&IC) Section 11464(c)(2)(A). The
COMPLETION AND SUBMISSION
Each county welfare department is responsible for ensuring that this report is fully and accurately completed. If portions of the report are completed by more than one entity within the County and/or outside agencies, the single contact person for each county responsible for submitting the one report to the state shall review the report for completeness and accuracy prior to submittal.
Counties that are licensed to provide adoption services will provide their AAP data to their county’s single contact person to submit in the county’s one report.
Counties that are not licensed to provide adoption services will receive their completed AAP paperwork from the CDSS Adoptions District Office that handles their county’s adoptions. The counties will then provide the AAP data to their single contact person to submit in the county’s one report.
Reports are to be received by the California Department of Social Services (CDSS) on or before the 30th calendar day of the month following the report quarter. The four report quarters for the state fiscal year are July through September, October through December, January through March, and April through June. This report may be submitted via
Hard copy submission: If
Page 1 of 6 |
STATE OF CALIFORNIA – HEALTH AND HUMAN SERVICES AGENCY |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
|
DATA SYSTEMS AND SURVEY DESIGN BUREAU |
COMPLETION AND SUBMISSION CONTINUED
California Department of Social Services
Data Systems and Survey Design Bureau, M.S.
P.O. Box 944243
Sacramento, CA
FAX: (916)
The report’s released quarterly statewide and
GENERAL INSTRUCTIONS
Enter in the boxes provided near the top of the form the county name, the version (Initial or Revised) and the report quarter and year.
Enter the data required for each item. If there is nothing to report for an item, enter “0”. Do not leave
any items blank.
Enter in the boxes at the end of the form the name, job title or classification, telephone number, extension, fax number, and
DEFINITIONS
AAP: Adoption Assistance Program (AAP) payments are monthly, per child cash payments to assist families that have adopted a special needs child from Foster Care.
Appeals: Appeals are filed regarding denials for new supplement to the rate requests or appeals are filed regarding denials for a change request on a previously authorized supplement to the rate request.
Authorized: The authorization of a new supplement to the rate request or an authorization for a change request for an existing previously authorized supplement to the rate.
California Regional Center: A California Regional Center is an agency that provides evaluations assessments, care management, and services for individuals with developmental disabilities who are residents of the State of California.
Change Requests: Change requests are requests to change a previously authorized supplement to the rate, e.g. asking that a Level II - $500 supplement to the rate amount be increased to a Level III - $750 supplement to the rate amount.
Children
Children (AAP): A child adopted from the foster care system and under 18 years of age, or under 21 years of age and has a mental or physical handicap that warrants the continuation of assistance.
Completed: A supplement to the rate request or supplement to the rate change request that has either been authorized or denied.
Page 2 of 6 |

STATE OF CALIFORNIA – HEALTH AND HUMAN SERVICES AGENCY |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
|
DATA SYSTEMS AND SURVEY DESIGN BUREAU |
DEFINITIONS CONTINUED
Denials: Denials are the supplement to the rate requests that are not authorized for any level and therefore determined not eligible for a supplement to the rate, or denials are supplement to the rate change requests that are not authorized for a different level.
Dual Agencies: The California Department of Social Services (CDSS) and the Department of Developmental Services (DDS).
Dual Agency Children: A dual agency child is a child in a foster care home, a child in adoptive placement, or adopted from the foster care system, who receives
Early Start Intervention Services, California: The California State Legislature passed the California Early Intervention Services Act (CEISA) in 1993 (CEISA; 14G.C. Section 95000, et seq.). CEISA established state authority to develop an early intervention service system that was congruent with federal requirements. DDS plans, develops, implements, and monitors the statewide early intervention services system in collaboration with the California Department of Education (CDE), and with the advice and assistance from the State Interagency Coordinating Council (ICC). The Departments of Health, Social Services, Mental Health, and Alcohol and Drug Programs cooperate and coordinate with DDS and CDE in the delivery of early intervention services.
Lanterman Act: The Lanterman Developmental Disabilities Act (AB 846), also known as the Lanterman Act, is a California law, initially proposed by Assembly Member Frank D. Lanterman in 1973 and passed in 1977, that gives people with developmental disabilities the right to services and supports that enable them to live a more independent and normal life.
Levels: The supplement to the rate structure has four levels established in increments of $250, $500, $750 and $1,000.
Supplement to the Rate: This is a supplement to the dual agency rate, broken into four levels, not to exceed one thousand dollars ($1,000) for dual agency children three years of age and older if it is determined the child has extraordinary care and supervision needs that cannot be met within the $2,006 dual agency rate.
ITEM INSTRUCTIONS
Each item must have entries from both of the programs serving dual agency children: the
Part A. Supplement to the Rate Requests for Dual Agency
1.Supplement to the rate requests carried forward from the last report quarter (Item 1a plus 1b): Enter the number of supplement to the rate requests carried over from the last report quarter. [CELLS 1 AND 2]
a.Pending supplement to the rate requests (Item 5 from the last report quarter): Enter the number of supplement to the rate requests pending at the end of the last report quarter. This must be the same number as in Item 5 (Cells 33 and 34) from the previous quarter’s report. [CELLS 3 AND 4]
Page 3 of 6 |
STATE OF CALIFORNIA – HEALTH AND HUMAN SERVICES AGENCY |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
|
DATA SYSTEMS AND SURVEY DESIGN BUREAU |
ITEM INSTRUCTIONS CONTINUED
b.Adjustment to Item 1a (positive or negative number), please explain in Comments: Skip this item if completing the Excel version; it will be automatically calculated. Enter any changes, plus
(+) or minus
2.New supplement to the rate requests received during the report quarter, by level (Items 2a plus 2b plus 2c plus 2d): Skip this item if completing the Excel version; it will be automatically calculated. Enter the total number of new supplement to the rate requests received during the report quarter.
[CELLS 7 AND 8]
a.Level I - $250: Enter the number of new $250 supplement to the rate requests received. [CELLS 9 AND 10]
b.Level II - $500: Enter the number of new $500 supplement to the rate requests received. [CELLS 11 AND 12]
c.Level III - $750: Enter the number of new $750 supplement to the rate requests received. [CELLS 13 AND 14]
d.Level IV - $1,000: Enter the number of new $1,000 supplement to the rate requests received. [CELLS 15 AND 16]
3.Total supplement to the rate requests on hand during the report quarter (Item 1 plus 2): Skip this item if completing the Excel version; it will be automatically calculated. It should equal the number of supplement to the rate requests on hand during the report quarter. This is the sum of Items 1 plus 2 (Cells 1 plus 7 and Cells 2 plus 8). [CELLS 17 AND 18]
4.Total supplement to the rate requests completed during the report quarter (Item 4a plus 4b): Skip this item if completing the Excel version; it will be automatically calculated. This is the sum of Items 4a plus 4b (Cells 21 plus 31 and Cells 22 plus 32). [CELLS 19 AND 20]
a.New supplement to the rate requests authorized during the report quarter, by level (Items 4a1 plus 4a2 plus 4a3 plus 4a4): Skip this item if completing the Excel version; it will be automatically calculated. Enter the total number of new supplement to the rate requests authorized during the report quarter by summing the four levels in each category (Cells 23, 25, 27, and 29 and Cells 24, 26, 28, and 30). [CELLS 21 AND 22]
1) Level I - $250: Enter the number of new $250 supplement to the rate requests authorized. [CELLS 23 AND 24]
2) Level II - $500: Enter the number of new $500 supplement to the rate requests authorized. [CELLS 25 AND 26]
3) Level III - $750: Enter the number of new $750 supplement to the rate requests authorized. [CELLS 27 AND 28]
4) Level IV - $1,000: Enter the number of new $1,000 supplement to the rate requests authorized. [CELLS 29 AND 30]
b.Supplement to the rate requests denied during the report quarter: Enter the total number of supplement to the rate requests denied during the report quarter. [CELLS 31 AND 32]
5.Total supplement to the rate requests pending at the end of the report quarter (Item 3 minus 4): Skip this item if completing the Excel version; it will be automatically calculated. Enter the total number of supplement to the rate requests remaining at the end of the quarter (Cell 17 minus Cell 19 and Cell 18 minus Cell 20). [CELLS 33 AND 34]
Page 4 of 6 |

STATE OF CALIFORNIA – HEALTH AND HUMAN SERVICES AGENCY |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
|
DATA SYSTEMS AND SURVEY DESIGN BUREAU |
ITEM INSTRUCTIONS CONTINUED
Part B. Appeals on Supplement to the Rate Requests
6.Appeals carried forward from the last report quarter (Item 6a plus 6b): Enter the number of appeals carried forward from the last report quarter. [CELLS 35 AND 36]
a.Pending appeals (Item 10 from the last report quarter): Enter the number of appeals pending from the last report quarter. This must be the same number as Item 10 (Cells 65 and 66) from the previous quarter’s report. [CELLS 37 AND 38]
b.Adjustment to Item 6a (positive or negative number), please explain in Comments: Skip this item if completing the Excel version; it will be automatically calculated. Enter any changes, plus
(+) or minus
7.New appeals received during the report quarter: Enter the total number of new appeals received during the report quarter. [CELLS 41 AND 42]
8.Total appeals on hand during the report quarter, by type (Item 6 plus 7; also Item 8a plus 8b plus 8c): Skip this item if completing the Excel version; it will be automatically calculated. This is the sum of Items 6 plus 7 (Cells 35 plus 41 and Cells 36 plus 42). Enter the total number of appeals on hand by type during the report quarter by summing the appeals in each category (Cells 45, 47 and 49 and Cells 46, 48 and 50). [CELLS 43 AND 44]
a.Change to child’s condition: Enter the number of appeals based on changes to a child’s condition. [CELLS 45 AND 46]
b.Provider disputing county denial: Enter the number of appeals by providers disputing a county denial. [CELLS 47 AND 48]
c.Provider seeking change to currently authorized supplement to the rate: Enter the number of appeals by providers seeking to change an existing supplement to the rate. [CELLS 49 AND 50]
9.Appeals completed during the report quarter (Items 9a plus 9b): Skip this item if completing the Excel version; it will be automatically calculated. Enter the total number of appeals completed during the report quarter by adding Items 9a plus 9b (Cells 53 and 63 and Cells 54 and 64).
[CELLS 51 AND 52]
a.Appeals authorized during the report quarter, by level (Items 9a1 plus 9a2 plus 9a3 plus 9a4): Skip this item if completing the Excel version; it will be automatically calculated. Enter the total number of appeals authorized during the report quarter by summing the four levels in each category. (Cells 55, 57, 59 and 61 and Cells 56, 58, 60 and 62). [CELLS 53 AND 54]
1)Level I - $250: Enter the number of appeals authorized for $250. [CELLS 55 AND 56]
2)Level II - $500: Enter the number of appeals authorized for $500. [CELLS 57 AND 58]
3)Level III - &750: Enter the number of appeals authorized for $750. [CELLS 59 AND 60]
4)Level IV - $1,000: Enter the number of appeals authorized for $1,000. [CELLS 61 AND 62]
b.Appeals on supplement to the rate requests denied during the report quarter: Enter the number of appeals on supplement to the rate requests denied during the report quarter.
[CELLS 63 AND 64]
Page 5 of 6 |
STATE OF CALIFORNIA – HEALTH AND HUMAN SERVICES AGENCY |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
|
DATA SYSTEMS AND SURVEY DESIGN BUREAU |
ITEM INSTRUCTIONS CONTINUED
10.Total appeals pending at the end of the report quarter (Item 8 minus Item 9): Skip this item if completing the Excel version; it will be automatically calculated. Enter the total number of appeals pending at the end of the report quarter (Cell 43 minus 51 and Cell 44 minus 52). [CELLS 65 AND 66]
COMMENTS
Use the Comments section to:
•Explain any adjustment entries [Item 1b (Cells 5 and 6); Item 6b (Cells 39 and 40)]
•Explain any major fluctuations in data.
•Provide information as directed in the report instructions.
•Provide any other comments the county determines necessary.
Page 6 of 6 |
Supplement to the Rate Requests for Dual Agency
and AAP Children
Quarterly Statistical Report VALIDATION RULES AND EDITS
CELLS 1 – 66: Data cells in this report must be greater than or equal to 0, except the adjustment entries (Cells 5, 6, 39 and 40) may be either a positive or negative number.
No data cells in either column should be left blank.
Part A. Supplement to the Rate Requests for Dual Agency
CELL 1 |
Cell 1 must equal (Cell 3 plus Cell 5) |
CELL 2 |
Cell 2 must equal (Cell 4 plus Cell 6) |
CELL 3 |
Cell 3 must equal Cell 33 from the previous quarter’s report |
CELL 4 |
Cell 4 must equal Cell 34 from the previous quarter’s report |
CELL 5 |
Cell 5 must equal (Cell 1 minus Cell 3) (may be a positive or negative number) |
CELL 6 |
Cell 6 must equal (Cell 2 minus Cell 4) (may be a positive or negative number) |
CELL 7 |
Cell 7 must equal (Cell 9 plus Cell 11 plus Cell 13 plus Cell 15) |
CELL 8 |
Cell 8 must equal (Cell 10 plus Cell 12 plus Cell 14 plus Cell 16) |
CELL 17 |
Cell 17 must equal (Cell 1 plus Cell 7) |
CELL 18 |
Cell 18 must equal (Cell 2 plus Cell 8) |
CELL 19 |
Cell 19 must equal (Cell 21 plus Cell 31) |
CELL 20 |
Cell 20 must equal (Cell 22 plus Cell 32) |
CELL 21 |
Cell 21 must equal (Cell 23 plus Cell 25 plus Cell 27 plus Cell 29) |
CELL 22 |
Cell 22 must equal (Cell 24 plus Cell 26 plus Cell 28 plus Cell 30) |
CELL 33 |
Cell 33 must equal (Cell 17 minus Cell 19) |
CELL 34 |
Cell 34 must equal (Cell 18 minus Cell 20) |
Part B. Appeals on Supplement to the Rate Requests |
|
CELL 35 |
Cell 35 must equal (Cell 37 plus Cell 39) |
CELL 36 |
Cell 36 must equal (Cell 38 plus Cell 40) |
CELL 37 |
Cell 37 must equal Cell 65 from the previous quarter’s report |
CELL 38 |
Cell 38 must equal Cell 66 from the previous quarter’s report |
CELL 39 |
Cell 39 must equal (Cell 35 minus Cell 37) (may be a positive or negative number) |
CELL 40 |
Cell 40 must equal (Cell 36 minus Cell 38) (may be a positive or negative number) |
CELL 43 |
Cell 43 must equal (Cell 35 plus Cell 41) |
|
Cell 43 must equal (Cell 45 plus Cell 47 plus Cell 49) |
CELL 44 |
Cell 44 must equal (Cell 36 plus Cell 42) |
|
Cell 44 must equal (Cell 46 plus Cell 48 plus Cell 50) |
CELL 51 |
Cell 51 must equal (Cell 53 plus Cell 63) |
CELL 52 |
Cell 52 must equal (Cell 54 plus Cell 64) |
CELL 53 |
Cell 53 must equal (Cell 55 plus Cell 57 plus Cell 59 plus Cell 61) |
CELL 54 |
Cell 54 must equal (Cell 56 plus Cell 58 plus Cell 60 plus Cell 62) |
CELL 65 |
Cell 65 must equal (Cell 43 minus Cell 51) |
CELL 66 |
Cell 66 must equal (Cell 44 minus Cell 52) |