
It is possible to fill in fda 1572 guidance easily by using our online editor for PDFs. To keep our tool on the forefront of practicality, we aim to put into operation user-oriented features and enhancements regularly. We are always looking for suggestions - join us in reshaping PDF editing. All it takes is a few easy steps:
Step 1: Open the PDF doc in our tool by hitting the "Get Form Button" in the top part of this page.
Step 2: Using this online PDF file editor, it is possible to do more than just complete forms. Edit away and make your documents appear perfect with customized textual content put in, or tweak the file's original input to perfection - all accompanied by the capability to add almost any images and sign it off.
It is an easy task to finish the form using out practical guide! Here is what you should do:
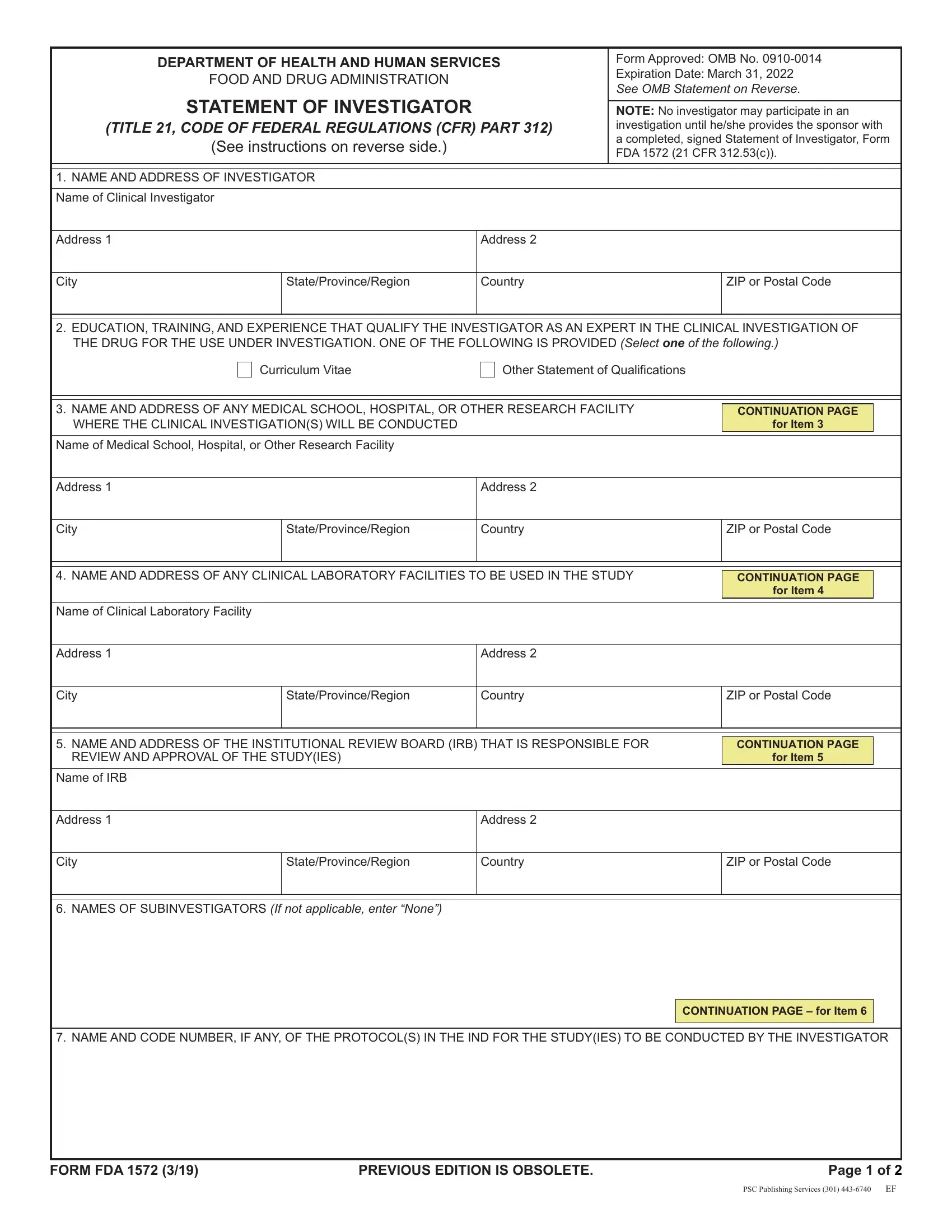
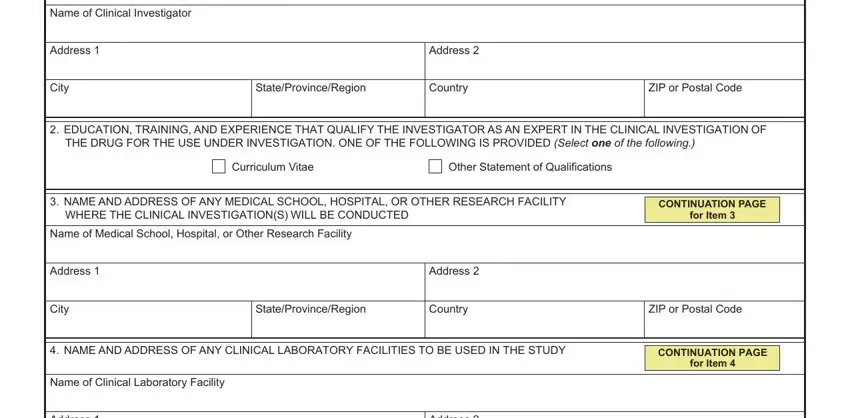
1. You will need to fill out the fda 1572 guidance accurately, so be careful when filling out the segments that contain these particular blank fields:
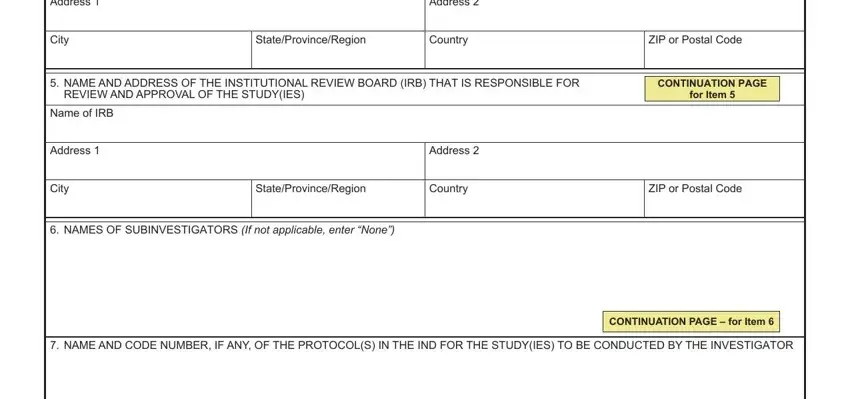
2. Your next part is usually to complete these fields: Address, City, Address, StateProvinceRegion, Country, ZIP or Postal Code, NAME AND ADDRESS OF THE, REVIEW AND APPROVAL OF THE STUDYIES, CONTINUATION PAGE, for Item, Name of IRB, Address, City, Address, and StateProvinceRegion.
3. This next step will be about PROVIDE THE FOLLOWING CLINICAL, For Phase investigations a, For Phase or investigations an, COMMITMENTS, I agree to conduct the studyies in, I agree to personally conduct or, I agree to inform any patients or, I agree to report to the sponsor, I agree to ensure that all, I agree to maintain adequate and, and I will ensure that an IRB that - fill out each one of these blank fields.
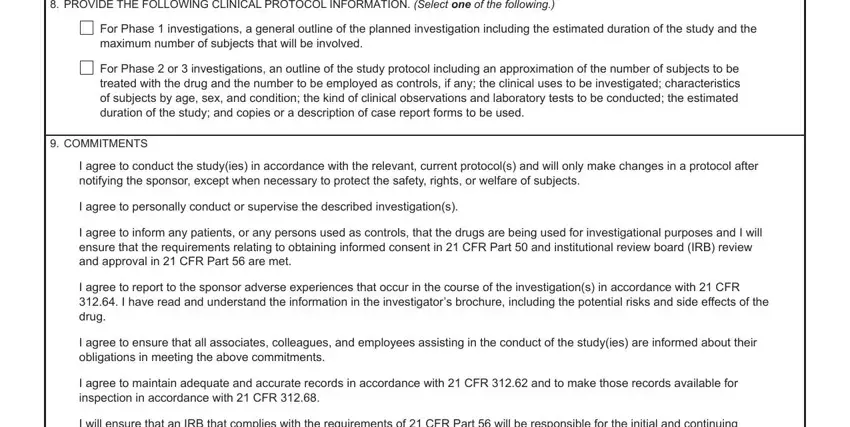
People frequently make mistakes while filling in COMMITMENTS in this area. Don't forget to re-examine everything you type in here.
4. Filling out DATE mmddyyyy, SIGNATURE OF INVESTIGATOR, Sign, WARNING A willfully false, The information below applies only, The burden time for this, Department of Health and Human, An agency may not conduct or, DO NOT SEND YOUR COMPLETED FORM TO, FORM FDA, PREVIOUS EDITION IS OBSOLETE, and Page of is essential in the next section - make sure to take your time and fill out each and every empty field!
Step 3: Immediately after double-checking the fields and details, click "Done" and you're good to go! Right after setting up a7-day free trial account with us, you will be able to download fda 1572 guidance or send it through email right away. The PDF will also be available in your personal account page with all your modifications. FormsPal provides protected document editing devoid of personal data recording or sharing. Feel comfortable knowing that your information is secure here!