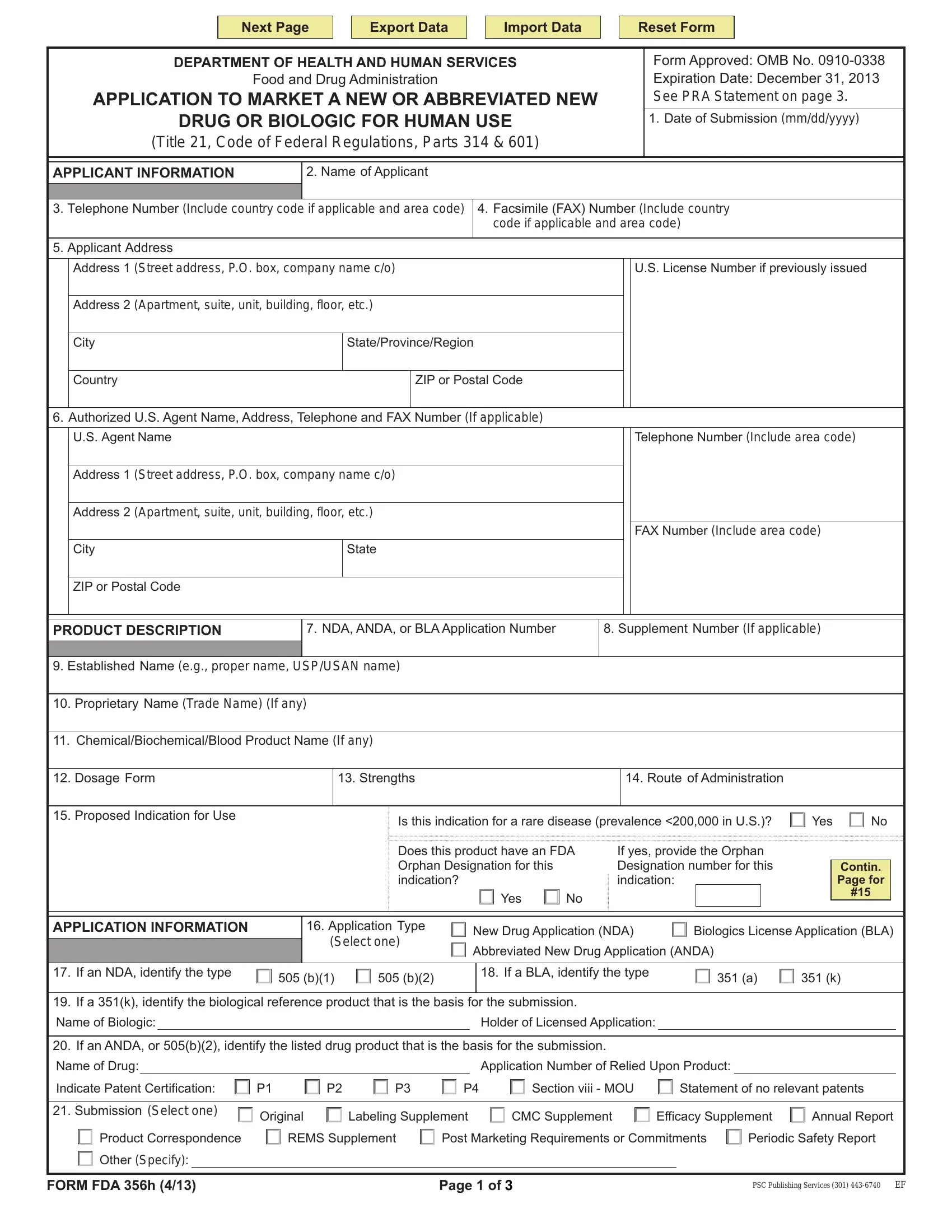
Navigating the complexities of introducing new or abbreviated drug and biologic products for human use in the United States involves a crucial step: completing and submitting the Form FDA 356h to the Food and Drug Administration (FDA). This form, under the auspices of the Department of Health and Human Services, gathers comprehensive details about the applicant, including contact information and addresses, and robust product descriptions ranging from the application number to the dosage form, strengths, route of administration, and proposed indications for use. Not only does it differentiate among New Drug Applications (NDAs), Biologics License Applications (BLAs), and Abbreviated New Drug Applications (ANDAs), but it also requires information on the type of submission, whether it's an original labeling, supplement, or a resubmission, alongside details about the manufacturing establishments involved. The form demands acknowledgment of the applicants' agreement to adhere to all applicable laws and regulations if the application is approved, including good manufacturing practices and labeling regulations. Applicants must certify the accuracy and truthfulness of the information provided, under penalty of law. Lastly, the form plays a role in regulatory frameworks beyond the FDA, stipulating compliance with local, state, and federal environmental impact laws and even touching upon scheduling under the Controlled Substances Act. Understanding the nuances of Form FDA 356h is essential for those seeking market approval for their pharmaceutical products in a highly regulated and competitive environment.
| Question | Answer |
|---|---|
| Form Name | Form Fda 356H |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | OMB, Rockville, is form 356h required for fda annual reports, is 356h required for annual report submissions |