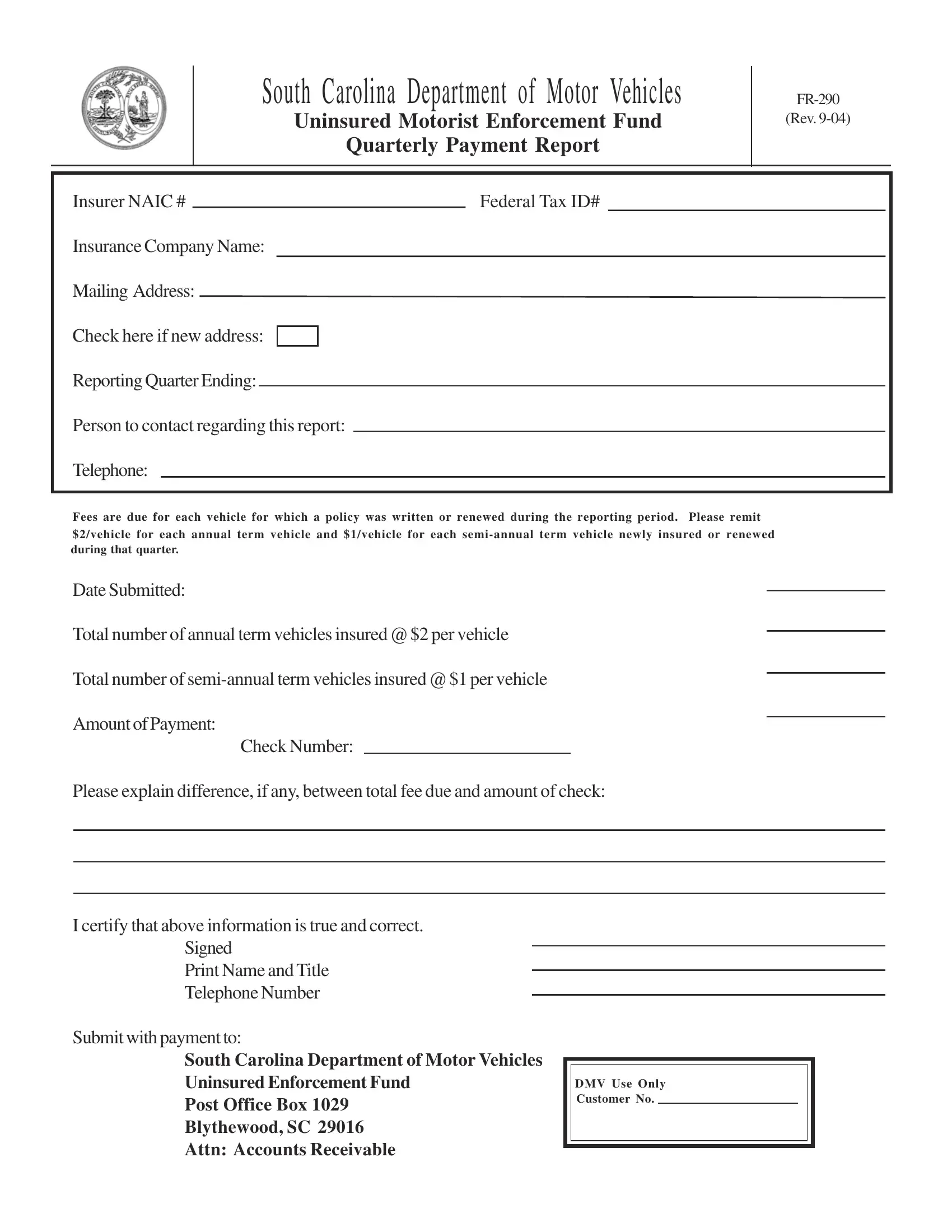
The financial framework that supports the Uninsured Motorist Enforcement Fund in South Carolina hinges on a pivotal document: the FR-290 form. Issued by the South Carolina Department of Motor Vehicles, this form serves as a quarterly payment report for insurers, meticulously detailing the fees due for vehicles they've insured or renewed within a given period. Specifically crafted to ensure compliance and support the state's efforts in managing uninsured motorists, the FR-290 form encapsulates vital information such as the insurer's NAIC number, federal tax ID, company name, and contact details, alongside a breakdown of fees per vehicle. These fees, modest yet crucial, amount to $2 for each vehicle on an annual term and $1 for those on a semi-annual term, underscoring the state's commitment to maintaining road safety and accountability. Furthermore, it emphasizes transparency and adherence to regulations by requiring a concise report on the number of vehicles insured, the total payment due, and a section for explaining any discrepancies between the expected and actual payment amounts. The process culminates in the certification of the report's accuracy, underscoring the collaborative efforts between insurers and the state government in mitigating the risks associated with uninsured drivers. As a cornerstone in the administration of the Uninsured Motorist Enforcement Fund, the FR-290 form embodies the procedural and financial responsibilities insurers bear, ensuring that each vehicle on the road contributes to a safer driving environment in South Carolina.
| Question | Answer |
|---|---|
| Form Name | Form Fr 290 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | FR 290 Form Revised 9 04 south carolina form fr 290 |
South Carolina Department of Motor Vehicles
Uninsured Motorist Enforcement Fund
Quarterly Payment Report
(Rev.
Insurer NAIC # |
Federal Tax ID# |
|||||
Insurance Company Name: |
|
|
||||
Mailing Address: |
|
|
||||
|
|
|
|
|
|
|
Check here if new address: |
|
|
|
|
||
Reporting Quarter Ending: |
|
|
|
|||
|
|
|
||||
Person to contact regarding this report: |
|
|
||||
Telephone: |
|
|
|
|||
|
|
|
|
|
|
|
Fees are due for each vehicle for which a policy was written or renewed during the reporting period. Please remit
$2/vehicle for each annual term vehicle and $1/vehicle for each
Date Submitted:
Total number of annual term vehicles insured @ $2 per vehicle
Total number of
Amount of Payment:
Check Number:
Please explain difference, if any, between total fee due and amount of check:
I certify that above information is true and correct.
Signed
Print Name and Title
Telephone Number
Submit with payment to:
South Carolina Department of Motor Vehicles
Uninsured Enforcement Fund
Post Office Box 1029
Blythewood, SC 29016
Attn: Accounts Receivable
DMV Use Only Customer No.