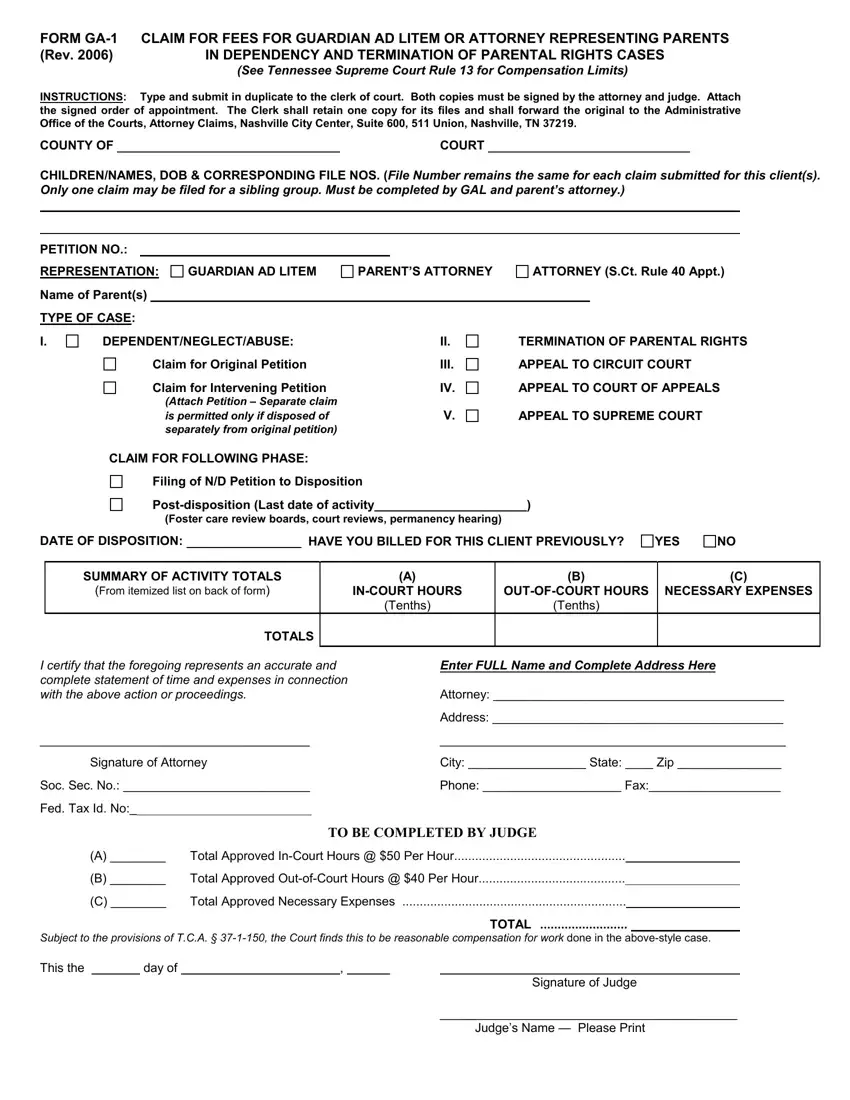
When navigating the complex terrain of legal representation in dependency and termination of parental rights cases, the Form GA-1 stands as a critical document. Initiated under the guidelines established by Tennessee Supreme Court Rule 13, which sets the compensation limits for legal professionals, this form delineates the process for claiming fees for Guardians Ad Litem or attorneys representing parents. Required to be typed and submitted in duplicate, it entails specific instructions that ensure a meticulous accounting of the legal work performed, involving both in-court and out-of-court hours, alongside necessary expenses incurred throughout the case. Each submission mandates the inclusion of a signed order of appointment, underscoring the necessity of official documentation. Furthermore, the form caters to a broad spectrum of case types—from dependency, neglect, and abuse, to various stages of appeals, hence providing a comprehensive framework for financial claims within the judicial system. Its structured format requires detailed activity summaries and emphasizes transparency and accountability by necessitating signatures from both the attorney involved and the presiding judge. Through this intricate process, the Form GA-1 serves not only as a procedural necessity but also as a testament to the structured approach adopted by the judiciary to oversee legal compensation in sensitive family law matters.
| Question | Answer |
|---|---|
| Form Name | Form Ga 1 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | termination of parental rights form georgia, signing over rights to child in georgia, termination of parental rights in georgia form, sign over parental rights forms georgia |
FORM
(Rev. 2006) |
IN DEPENDENCY AND TERMINATION OF PARENTAL RIGHTS CASES |
|
(See Tennessee Supreme Court Rule 13 for Compensation Limits) |
INSTRUCTIONS: Type and submit in duplicate to the clerk of court. Both copies must be signed by the attorney and judge. Attach the signed order of appointment. The Clerk shall retain one copy for its files and shall forward the original to the Administrative Office of the Courts, Attorney Claims, Nashville City Center, Suite 600, 511 Union, Nashville, TN 37219.
COUNTY OF |
|
COURT |
CHILDREN/NAMES, DOB & CORRESPONDING FILE NOS. (File Number remains the same for each claim submitted for this client(s). Only one claim may be filed for a sibling group. Must be completed by GAL and parent’s attorney.)
PETITION NO.:
REPRESENTATION:
Name of Parent(s)
TYPE OF CASE:
GUARDIAN AD LITEM
PARENT’S ATTORNEY
ATTORNEY (S.Ct. Rule 40 Appt.)
I.
DEPENDENT/NEGLECT/ABUSE: |
II. |
Claim for Original Petition |
III. |
Claim for Intervening Petition |
IV. |
(Attach Petition – Separate claim |
|
is permitted only if disposed of |
V. |
separately from original petition) |
|
CLAIM FOR FOLLOWING PHASE: |
|
Filing of N/D Petition to Disposition |
|
TERMINATION OF PARENTAL RIGHTS
APPEAL TO CIRCUIT COURT
APPEAL TO COURT OF APPEALS
APPEAL TO SUPREME COURT
(Foster care review boards, court reviews, permanency hearing)
DATE OF DISPOSITION: |
|
HAVE YOU BILLED FOR THIS CLIENT PREVIOUSLY? |
YES
NO
|
SUMMARY OF ACTIVITY TOTALS |
|
(A) |
(B) |
(C) |
|
(From itemized list on back of form) |
|
NECESSARY EXPENSES |
||
|
|
|
(Tenths) |
(Tenths) |
|
|
TOTALS |
|
|
|
|
|
|
|
|
|
|
I certify that the foregoing represents an accurate and |
Enter FULL Name and Complete Address Here |
||||
complete statement of time and expenses in connection |
|
|
|
||
with the above action or proceedings. |
Attorney: __________________________________________ |
||||
|
|
|
Address: __________________________________________ |
||
_______________________________________ |
|
__________________________________________________ |
|||
|
Signature of Attorney |
City: _________________ State: ____ Zip _______________ |
|||
Soc. Sec. No.: ___________________________ |
Phone: ____________________ Fax:___________________ |
||||
Fed. Tax Id. No:_____________________________
|
TO BE COMPLETED BY JUDGE |
(A) ________ |
Total Approved |
(B) ________ |
Total Approved |
(C) ________ |
Total Approved Necessary Expenses |
TOTAL .........................
Subject to the provisions of T.C.A. §
This the |
|
day of |
|
, |
Signature of Judge
___________________________________________
Judge’s Name — Please Print
DATE
ACTIVITY
Itemize
Itemize any other approved expenses & attach to the back of this claim a certified copy of the court=s prior approval of such expense.
(A)
HOURS (Tenths)
(B)
(C)
NECESSARY EXPENSES
Continued on next page…
(Right click on number and select “update field” to calculate) TOTALS:
0
0
$ 0.00
