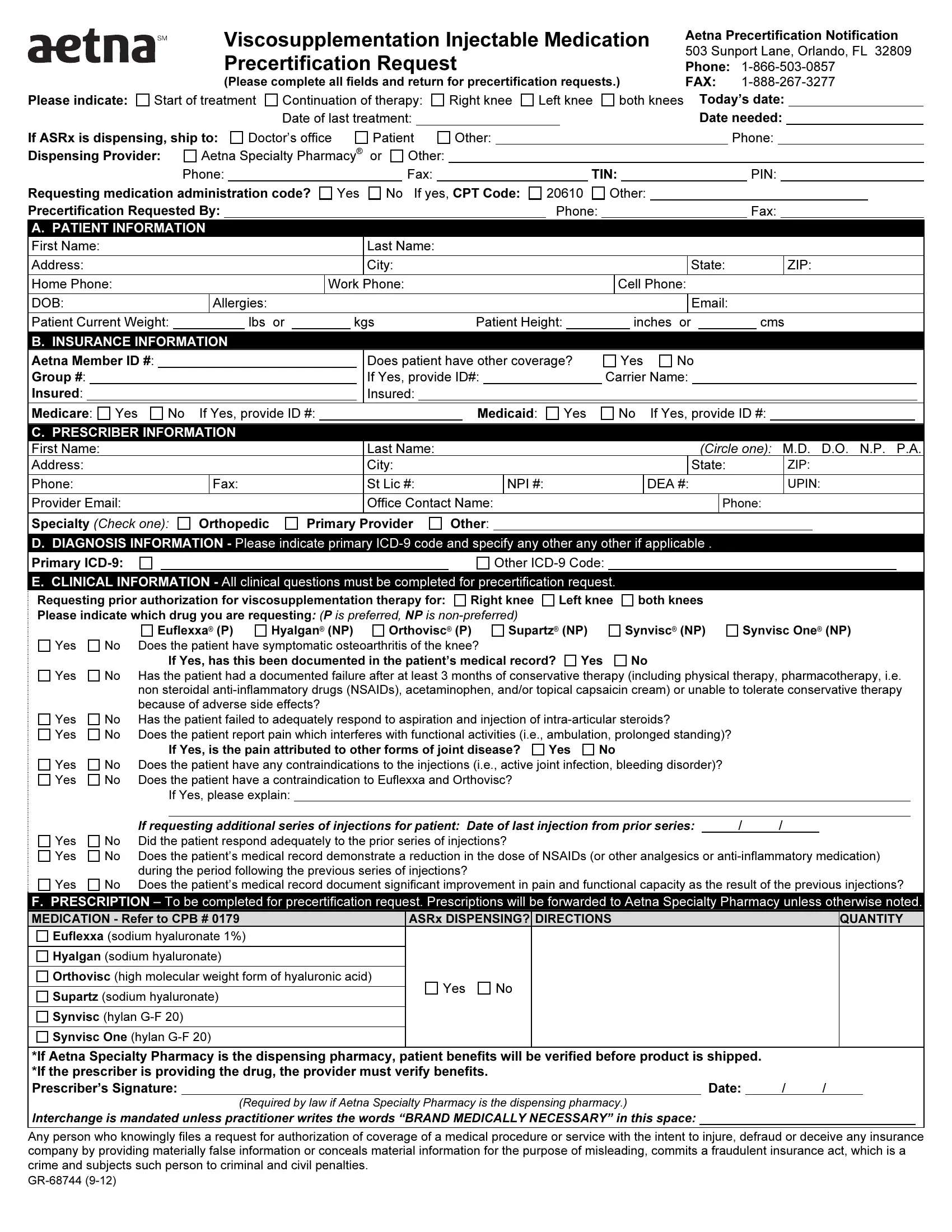
In the realm of healthcare, managing the complexities of therapy and medication authorization is a task that requires meticulous attention to detail and thoroughness. The GR 68744 form stands as a crucial document for practitioners and patients navigating the process of precertification for viscosupplementation injectable medications under Aetna's guidelines. Located at 503 Sunport Lane in Orlando, Florida, this document is essential for those seeking approval for treatments aimed at alleviating symptoms associated with knee osteoarthritis. It meticulously outlines the need for complete information regarding the patient's medical and insurance details, the prescriber's credentials, and detailed clinical information justifying the request for viscosupplementation therapy. Whether for the initiation or continuation of treatment, the form seeks to streamline the process by requesting data on the patient’s condition, prior treatments, and the specific medication sought, be it Euflexxa, Hyalgan, Orthovisc, Supartz, Synvisc, or Synvisc One. Additional sections emphasize the clinical rationale behind the therapy request, documenting the patient's osteoarthritis symptoms, their response to conservative treatments, and any contraindications to the suggested therapy. The form underscores the collaborative effort between healthcare providers and insurance entities, aiming to ensure that patients receive optimal care tailored to their specific needs through a transparent and efficient authorization process.
| Question | Answer |
|---|---|
| Form Name | Form Gr 68744 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ICD-9, aetna form gr 68744, Orlando, aetna gr 68744 form printable |
Viscosupplementation Injectable Medication |
Aetna Precertification Notification |
||
503 Sunport Lane, Orlando, FL 32809 |
|||
Precertification Request |
|||
Phone: |
|||
(Please complete all fields and return for precertification requests.) |
FAX: |
||
Please indicate: Start of treatment Continuation of therapy:
Right knee
Left knee
both knees Today’s date:
|
|
|
|
|
|
|
|
|
|
|
Date of last treatment: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date needed: |
|
|||||||||||||||||||||
If ASRx is dispensing, ship to: |
Doctor’s office |
Patient |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|||||||||||||||||||||||||||||||||||
Dispensing Provider: |
|
|
Aetna Specialty Pharmacy® |
or |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
Phone: |
|
|
|
|
|
|
|
|
|
|
Fax: |
|
|
|
|
|
|
|
|
|
|
TIN: |
|
|
|
|
|
|
|
|
PIN: |
|
||||||||||||||||||
Requesting medication administration code? |
Yes |
No |
If yes, CPT Code: |
20610 |
|
|
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
Precertification Requested By: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax: |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
A. PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
|
|
|
|
ZIP: |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Home Phone: |
|
|
|
|
|
|
|
|
|
|
Work Phone: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cell Phone: |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
DOB: |
|
|
|
Allergies: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Email: |
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Patient Current Weight: |
|
|
|
|
|
lbs |
or |
|
|
kgs |
|
|
|
|
|
Patient Height: |
|
|
|
|
|
inches or |
|
|
|
cms |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
B. INSURANCE INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Aetna Member ID #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Does patient have other coverage? |
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
Group #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If Yes, provide ID#: |
|
|
|
|
|
|
Carrier Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
Insured: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insured: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
Medicare: Yes |
No |
If Yes, provide ID #: |
|
|
|
|
|
|
|
|
|
|
Medicaid: |
|
Yes |
|
|
No |
|
If Yes, provide ID #: |
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
C. PRESCRIBER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(CIRCLE ONE): M.D. D.O. N.P. P.A. |
||||||||||||||||||||
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State: |
|
|
|
|
|
|
ZIP: |
|||||||||||
Phone: |
|
|
|
Fax: |
|
|
|
|
|
|
|
St Lic #: |
|
|
|
|
|
NPI #: |
|
|
|
|
|
|
|
|
|
|
DEA #: |
|
|
|
|
|
|
UPIN: |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
Provider Email: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Office Contact Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone: |
|||||||||||||||||||||||||
Specialty (CHECK ONE): |
Orthopedic |
|
Primary Provider |
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D.DIAGNOSIS INFORMATION - Please indicate primary
Primary |
|
Other |
E.CLINICAL INFORMATION - All clinical questions must be completed for precertification request.
Requesting prior authorization for viscosupplementation therapy for: |
Right knee |
Left knee |
both knees |
|
|||||||
Please indicate which drug you are requesting: (P is preferred, NP is |
|
|
|
|
|||||||
|
|
Euflexxa® (P) |
Hyalgan® (NP) |
Orthovisc® (P) |
Supartz® (NP) |
Synvisc® (NP) |
Synvisc One® (NP) |
||||
Yes |
No |
Does the patient have symptomatic osteoarthritis of the knee? |
|
|
|
|
|
||||
|
|
If Yes, has this been documented in the patient’s medical record? |
Yes |
No |
|
||||||
Yes |
No |
Has the patient had a documented failure after at least 3 months of conservative therapy (including physical therapy, pharmacotherapy, i.e. |
|||||||||
|
|
non steroidal |
|||||||||
|
|
because of adverse side effects? |
|
|
|
|
|
|
|
||
Yes |
No |
Has the patient failed to adequately respond to aspiration and injection of |
|
||||||||
Yes |
No |
Does the patient report pain which interferes with functional activities (i.e., ambulation, prolonged standing)? |
|
||||||||
|
|
If Yes, is the pain attributed to other forms of joint disease? |
Yes |
No |
|
|
|||||
Yes |
No |
Does the patient have any contraindications to the injections (i.e., active joint infection, bleeding disorder)? |
|
||||||||
Yes |
No |
Does the patient have a contraindication to Euflexxa and Orthovisc? |
|
|
|
|
|||||
|
|
If Yes, please explain: |
|
|
|
|
|
|
|
|
|
Yes Yes
Yes
|
If requesting additional series of injections for patient: Date of last injection from prior series: |
/ |
/ |
|
No |
Did the patient respond adequately to the prior series of injections? |
|
|
|
No |
Does the patient’s medical record demonstrate a reduction in the dose of NSAIDs (or other analgesics or |
|||
|
during the period following the previous series of injections? |
|
|
|
No |
Does the patient’s medical record document significant improvement in pain and functional capacity as the result of the previous injections? |
|||
F.PRESCRIPTION – To be completed for precertification request. Prescriptions will be forwarded to Aetna Specialty Pharmacy unless otherwise noted.
MEDICATION - Refer to CPB # 0179 |
ASRx DISPENSING? |
DIRECTIONS |
||
Euflexxa (sodium hyaluronate 1%) |
|
|
|
|
|
|
|
|
|
Hyalgan (sodium hyaluronate) |
|
|
|
|
|
|
|
|
|
Orthovisc (high molecular weight form of hyaluronic acid) |
Yes |
No |
|
|
|
|
|||
Supartz (sodium hyaluronate) |
||||
|
|
|
||
|
|
|
|
|
Synvisc (hylan |
|
|
|
|
|
|
|
|
|
Synvisc One (hylan |
|
|
|
|
|
|
|
|
|
QUANTITY
*If Aetna Specialty Pharmacy is the dispensing pharmacy, patient benefits will be verified before product is shipped. |
|
|
|
*If the prescriber is providing the drug, the provider must verify benefits. |
|
|
|
Prescriber’s Signature: |
Date: |
/ |
/ |
(Required by law if Aetna Specialty Pharmacy is the dispensing pharmacy.)
Interchange is mandated unless practitioner writes the words “BRAND MEDICALLY NECESSARY” in this space:
Any person who knowingly files a request for authorization of coverage of a medical procedure or service with the intent to injure, defraud or deceive any insurance company by providing materially false information or conceals material information for the purpose of misleading, commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.