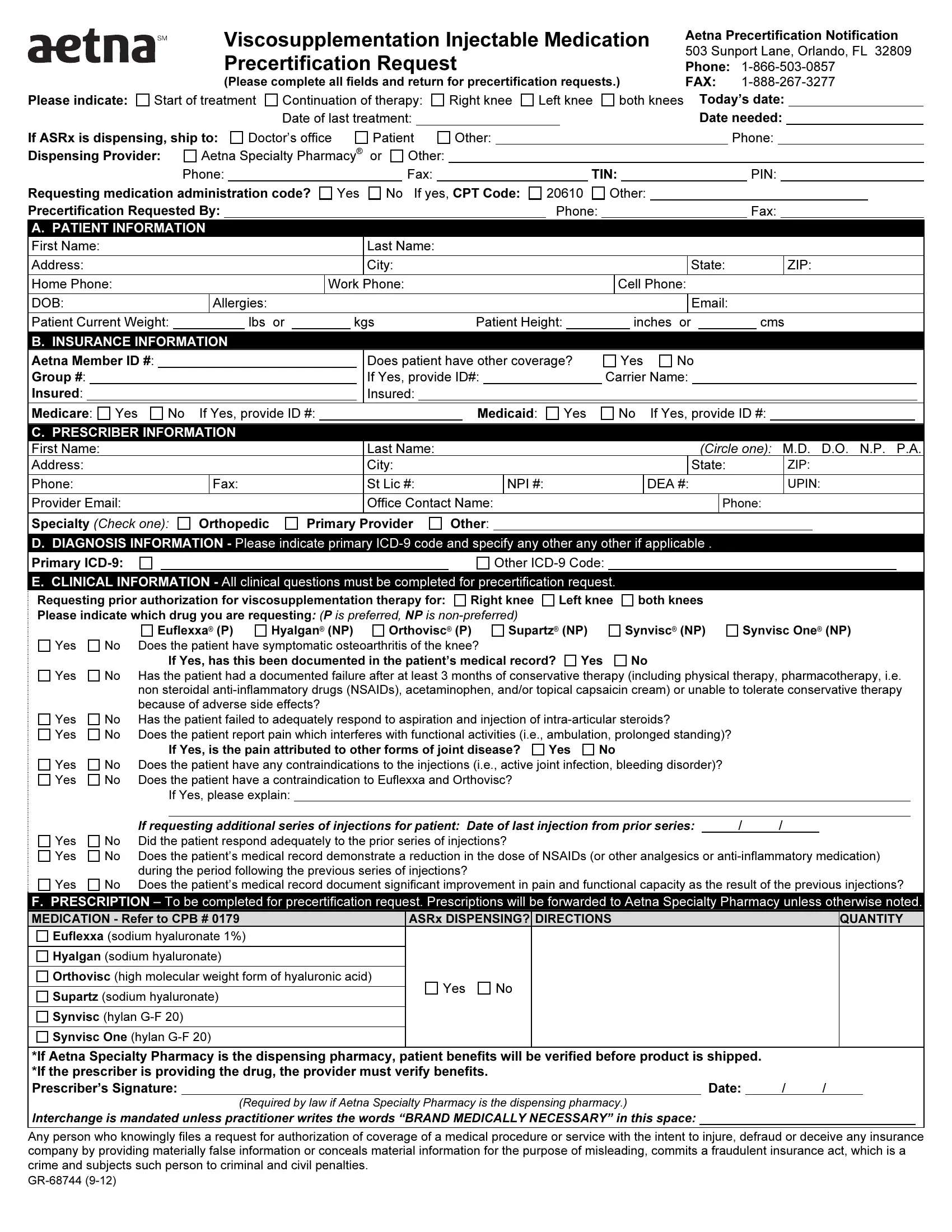
In the realm of healthcare, managing the complexities of therapy and medication authorization is a task that requires meticulous attention to detail and thoroughness. The GR 68744 form stands as a crucial document for practitioners and patients navigating the process of precertification for viscosupplementation injectable medications under Aetna's guidelines. Located at 503 Sunport Lane in Orlando, Florida, this document is essential for those seeking approval for treatments aimed at alleviating symptoms associated with knee osteoarthritis. It meticulously outlines the need for complete information regarding the patient's medical and insurance details, the prescriber's credentials, and detailed clinical information justifying the request for viscosupplementation therapy. Whether for the initiation or continuation of treatment, the form seeks to streamline the process by requesting data on the patient’s condition, prior treatments, and the specific medication sought, be it Euflexxa, Hyalgan, Orthovisc, Supartz, Synvisc, or Synvisc One. Additional sections emphasize the clinical rationale behind the therapy request, documenting the patient's osteoarthritis symptoms, their response to conservative treatments, and any contraindications to the suggested therapy. The form underscores the collaborative effort between healthcare providers and insurance entities, aiming to ensure that patients receive optimal care tailored to their specific needs through a transparent and efficient authorization process.
| Question | Answer |
|---|---|
| Form Name | Form Gr 68744 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ICD-9, aetna form gr 68744, Orlando, aetna gr 68744 form printable |
