
form 0960 0269 can be completed online very easily. Simply use FormsPal PDF tool to get the job done quickly. FormsPal professional team is continuously working to improve the editor and help it become much easier for people with its cutting-edge functions. Discover an constantly innovative experience today - explore and discover new possibilities along the way! To get the ball rolling, take these basic steps:
Step 1: Click the "Get Form" button above. It's going to open up our tool so you could begin filling out your form.
Step 2: After you open the PDF editor, you'll see the document made ready to be completed. Aside from filling in various blank fields, you could also perform other actions with the file, such as adding any text, editing the initial textual content, inserting graphics, affixing your signature to the document, and much more.
As for the blanks of this specific PDF, this is what you should know:
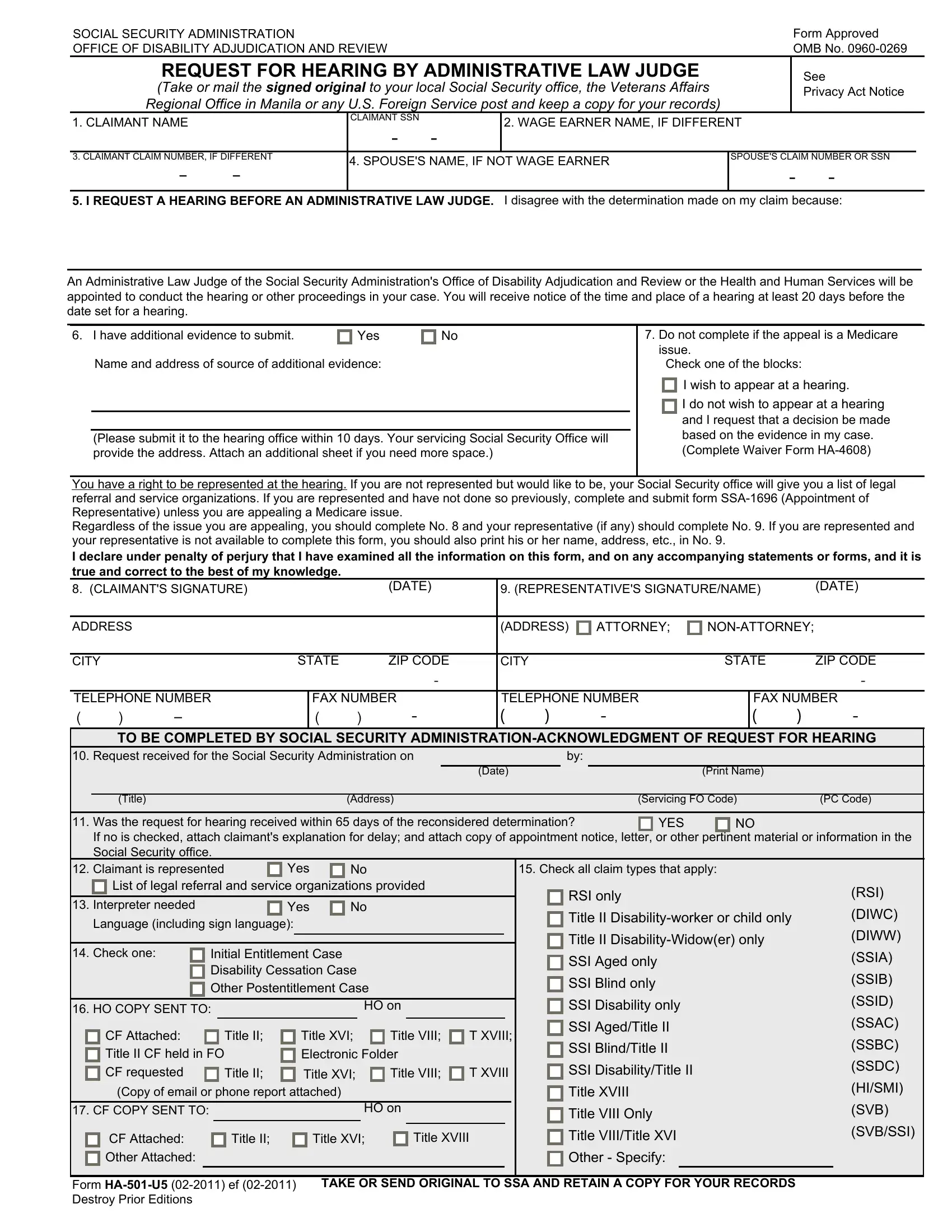
1. When completing the form 0960 0269, be sure to complete all of the important blanks in their corresponding section. This will help to hasten the work, enabling your details to be handled efficiently and appropriately.
2. The subsequent step is to fill out these particular fields: CITY, STATE, ZIP CODE, CITY, STATE, ZIP CODE, TELEPHONE NUMBER, FAX NUMBER, TELEPHONE NUMBER, FAX NUMBER, TO BE COMPLETED BY SOCIAL SECURITY, Request received for the Social, Date, Print Name, and Title.
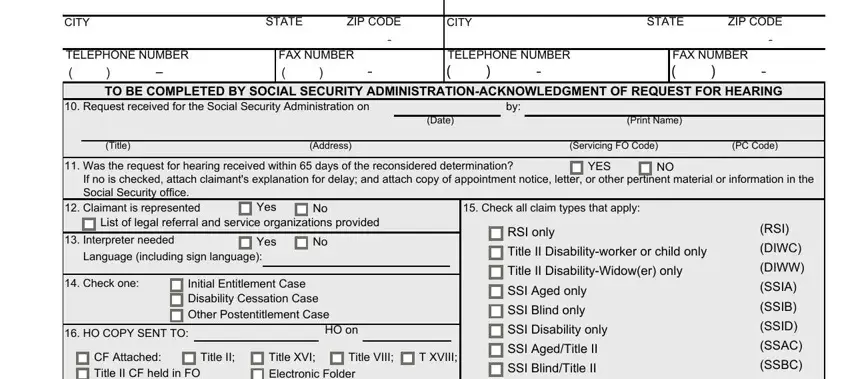
Be very attentive while completing CITY and CITY, since this is the section in which a lot of people make errors.
Step 3: After taking one more look at your fields and details, press "Done" and you are done and dusted! Sign up with us right now and easily access form 0960 0269, prepared for download. Each change you make is handily kept , meaning you can customize the pdf at a later point if required. FormsPal ensures your information confidentiality by using a protected method that in no way saves or shares any private information used in the file. Be confident knowing your files are kept safe whenever you work with our tools!