 PHYSICIAN OR SUPPLIER INFORMATION
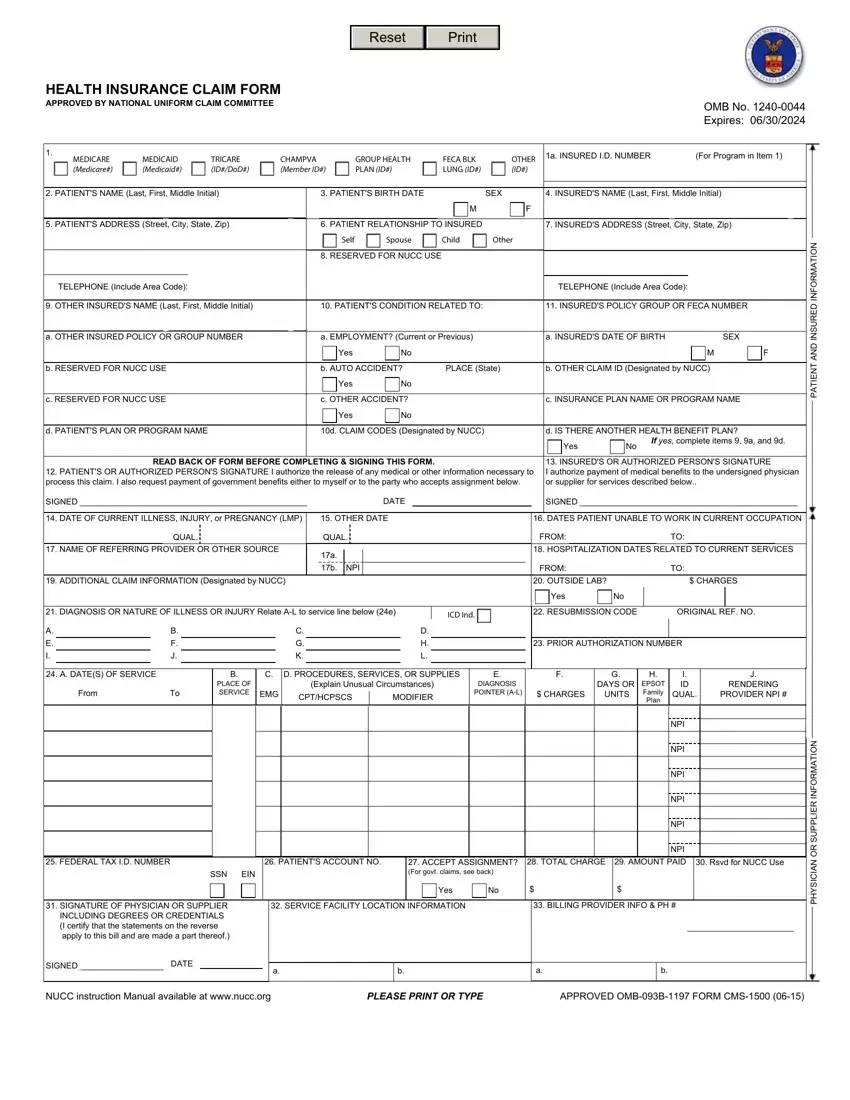
PHYSICIAN OR SUPPLIER INFORMATIONFilling out how to form insurance claim fill out is a snap. Our experts designed our tool to really make it intuitive and allow you to fill out any PDF online. Below are a few steps that you should stick to:
Step 1: Choose the "Get Form Now" button to get started on.
Step 2: So, you're on the file editing page. You may add information, edit present data, highlight specific words or phrases, insert crosses or checks, add images, sign the form, erase unwanted fields, etc.
These segments will help make up the PDF form:
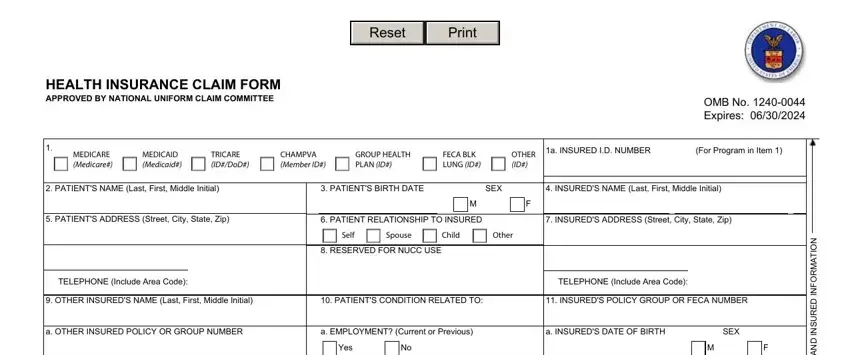
Within the field b RESERVED FOR NUCC USE, b AUTO ACCIDENT, PLACE State, b OTHER CLAIM ID Designated by NUCC, c RESERVED FOR NUCC USE, Yes, c OTHER ACCIDENT, Yes, c INSURANCE PLAN NAME OR PROGRAM, d PATIENTS PLAN OR PROGRAM NAME, d CLAIM CODES Designated by NUCC, d IS THERE ANOTHER HEALTH BENEFIT, Yes, If yes complete items a and d, and READ BACK OF FORM BEFORE type in the data which the program requires you to do.
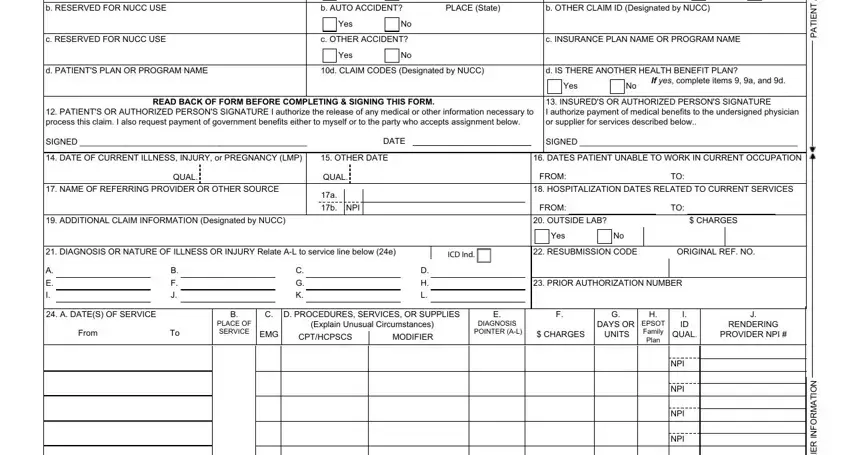
Put in writing any details you need inside the area NPI, NPI, FEDERAL TAX ID NUMBER, PATIENTS ACCOUNT NO, SSN, EIN, ACCEPT ASSIGNMENT For govt claims, TOTAL CHARGE, AMOUNT PAID, Rsvd for NUCC Use, SIGNATURE OF PHYSICIAN OR, SIGNED DATE, SERVICE FACILITY LOCATION, BILLING PROVIDER INFO PH, and Yes.
Step 3: Click the "Done" button. Next, you may transfer your PDF document - download it to your device or send it by means of email.
Step 4: Make at least a couple of copies of your file to refrain from different upcoming challenges.
