In the state of Florida, individuals have the opportunity to take charge of their future medical care through the use of a Health Care Surrogate form, as outlined in Section 765.203 of the Florida Statutes. This legal document enables a person to designate someone else, a health care surrogate, to make medical decisions on their behalf in the event they are unable to do so themselves. The form provides a structured way to specify one’s choice for a surrogate, along with an alternate, ensuring that decisions regarding health care can be made by a trusted individual when necessary. It enables the surrogate to access the principal's health information and make all types of health care decisions, ranging from providing informed consent to making decisions about anatomical gifts. Importantly, this designation can include specific instructions and restrictions, tailoring the authority of the surrogate to the individual’s preferences. While the principal retains decision-making capacity, their own decisions take precedence, and they are kept informed of any decisions made by the surrogate. It is crucial to note that the authority of the health care surrogate is not diminished by the principal’s subsequent incapacity, ensuring continuity of care and decision-making. The form also outlines the conditions under which the surrogate’s authority becomes effective and how one might revoke or amend the designation. Crafted to uphold the rights and wishes of individuals regarding their health care, the Florida Health Care Surrogate form is a key legal tool in planning for future health care needs.
| Question | Answer |
|---|---|
| Form Name | Florida Health Care Surrogate Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | printable fl health care surrogate form, health care surrogate form pdf, health proxy form florida, designation of health care surrogate document |
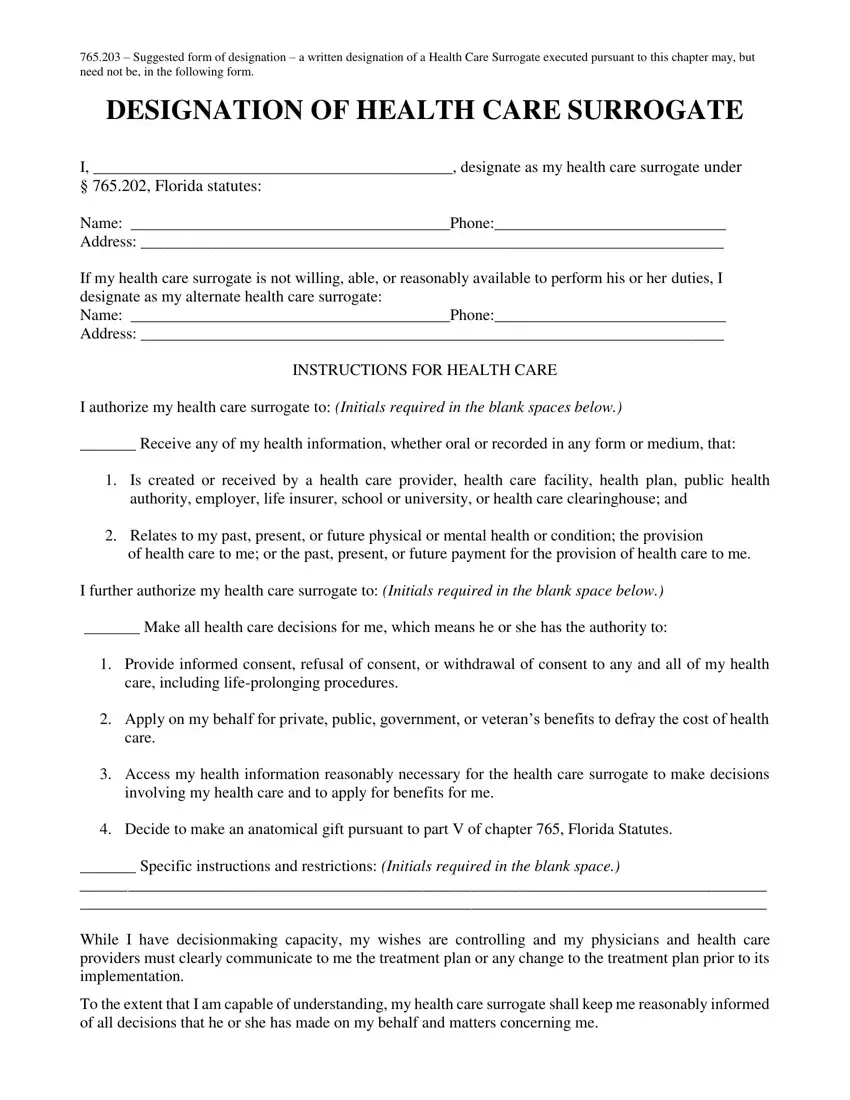
765.203 – Suggested form of designation – a written designation of a Health Care Surrogate executed pursuant to this chapter may, but need not be, in the following form.
DESIGNATION OF HEALTH CARE SURROGATE
I, _____________________________________________, designate as my health care surrogate under
§ 765.202, Florida statutes:
Name: ________________________________________Phone:_____________________________
Address: _________________________________________________________________________
If my health care surrogate is not willing, able, or reasonably available to perform his or her duties, I designate as my alternate health care surrogate:
Name: ________________________________________Phone:_____________________________
Address: _________________________________________________________________________
INSTRUCTIONS FOR HEALTH CARE
I authorize my health care surrogate to: (Initials required in the blank spaces below.)
_______ Receive any of my health information, whether oral or recorded in any form or medium, that:
1.Is created or received by a health care provider, health care facility, health plan, public health authority, employer, life insurer, school or university, or health care clearinghouse; and
2.Relates to my past, present, or future physical or mental health or condition; the provision
of health care to me; or the past, present, or future payment for the provision of health care to me.
I further authorize my health care surrogate to: (Initials required in the blank space below.)
_______ Make all health care decisions for me, which means he or she has the authority to:
1.Provide informed consent, refusal of consent, or withdrawal of consent to any and all of my health care, including
2.Apply on my behalf for private, public, government, or veteran’s benefits to defray the cost of health care.
3.Access my health information reasonably necessary for the health care surrogate to make decisions involving my health care and to apply for benefits for me.
4.Decide to make an anatomical gift pursuant to part V of chapter 765, Florida Statutes.
_______ Specific instructions and restrictions: (Initials required in the blank space.)
______________________________________________________________________________________
______________________________________________________________________________________
While I have decisionmaking capacity, my wishes are controlling and my physicians and health care providers must clearly communicate to me the treatment plan or any change to the treatment plan prior to its implementation.
To the extent that I am capable of understanding, my health care surrogate shall keep me reasonably informed of all decisions that he or she has made on my behalf and matters concerning me.
THIS HEALTH CARE SURROGATE DESIGNATION IS NOT AFFECTED BY MY SUBSEQUENT INCAPACITY EXCEPT AS PROVIDED IN CHAPTER 765, FLORIDA STATUTES.
PURSUANT TO SECTION 765.104, FLORIDA STATUTES, I UNDERSTAND THAT I MAY, AT ANY TIME WHILE I RETAIN MY CAPACITY, REVOKE OR AMEND THIS DESIGNATION BY:
1.SIGNING A WRITTEN AND DATED INSTRUMENT WHICH EXPRESSES MY INTENT TO AMEND OR REVOKE THIS DESIGNATION;
2.PHYSICALLY DESTROYING THIS DESIGNATION THROUGH MY OWN ACTION OR BY THAT OF ANOTHER PERSON IN MY PRESENCE AND UNDER MY DIRECTION;
3.VERBALLY EXPRESSING MY INTENTION TO AMEND OR REVOKE THIS DESIGNATION; OR
4.SIGNING A NEW DESIGNATION THAT IS MATERIALLY DIFFERENT FROM THIS DESIGNATION.
MY HEALTH CARE SURROGATE’S AUTHORITY BECOMES EFFECTIVE WHEN MY PRIMARY PHYSICIAN DETERMINES THAT I AM UNABLE TO MAKE MY OWN HEALTH CARE DECISIONS UNLESS I INITIAL EITHER OR BOTH OF THE FOLLOWING BOXES:
IF I INITIAL THIS BOX [_______] MY HEALTH CARE SURROGATE’S AUTHORITY TO RECEIVE
MY HEALTH INFORMATION TAKES EFFECT IMMEDIATELY.
IF I INITIAL THIS BOX [_______] MY HEALTH CARE SURROGATE’S AUTHORITY TO MAKE
HEALTH CARE DECISIONS FOR ME TAKES EFFECT IMMEDIATELY. PURSUANT TO SECTION 765.204(3), FLORIDA STATES, ANY INSTRUCTIONS OF HEALTH CARE DECISIONS I MAKE,
EITHER VERBALLY OR IN WRITING, WHILE I POSSESS CAPACITY SHALL SUPERCEDE ANY INSTRUCTIONS OR HEALTH CARE DECISIONS MADE BY MY SURROGATE THAT ARE IN MATERIAL CONFLICT WITH THOSE MADE BY ME.
Signature: Sign and date the form here:
_________________ ______________________________ _______________________________
DateSignaturePrinted Name
_________________________________________________________________________________
Address
Signatures of Witnesses:
Witness:_________________________________ Witness:_________________________________
Printed Name: ____________________________ Printed Name: ____________________________
Address: ________________________________ Address: ________________________________
_________________________________________________________________
Phone: _________________________________ Phone: ___________________________________
Source: The 2016 Florida Statutes, Title XLIV, CIVIL RIGHTS, Chapter 765. Health Care Directives 765.203 Suggested Form of Designation ©
