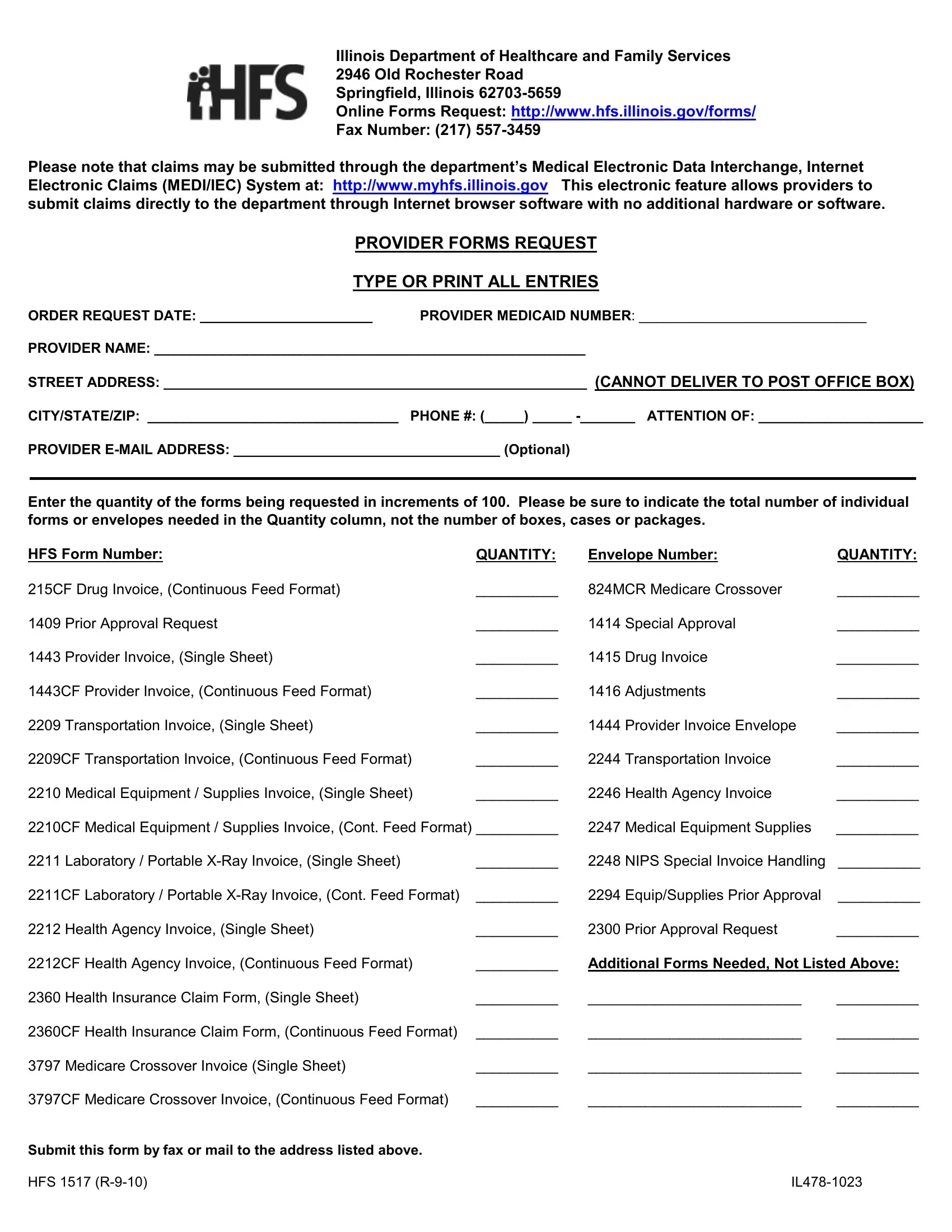
Illinois Department of Healthcare and Family Services
2946 Old Rochester Road
Springfield, Illinois 62703-5659
Online Forms Request: http://www.hfs.illinois.gov/forms/
Fax Number: (217) 557-3459
Please note that claims may be submitted through the department’s Medical Electronic Data Interchange, Internet Electronic Claims (MEDI/IEC) System at: http://www.myhfs.illinois.gov This electronic feature allows providers to submit claims directly to the department through Internet browser software with no additional hardware or software.
PROVIDER FORMS REQUEST
TYPE OR PRINT ALL ENTRIES
ORDER REQUEST DATE: ______________________ PROVIDER MEDICAID NUMBER: _____________________________
PROVIDER NAME: _______________________________________________________
STREET ADDRESS: ______________________________________________________ (CANNOT DELIVER TO POST OFFICE BOX)
CITY/STATE/ZIP: ________________________________ PHONE #: (_____) _____ -_______ ATTENTION OF: _____________________
PROVIDER E-MAIL ADDRESS: __________________________________ (Optional)
Enter the quantity of the forms being requested in increments of 100. Please be sure to indicate the total number of individual forms or envelopes needed in the Quantity column, not the number of boxes, cases or packages.
HFS Form Number: |
QUANTITY: |
Envelope Number: |
QUANTITY: |
215CF Drug Invoice, (Continuous Feed Format) |
__________ |
824MCR Medicare Crossover |
__________ |
1409 |
Prior Approval Request |
__________ |
1414 |
Special Approval |
__________ |
1443 |
Provider Invoice, (Single Sheet) |
__________ |
1415 |
Drug Invoice |
__________ |
1443CF Provider Invoice, (Continuous Feed Format) |
__________ |
1416 |
Adjustments |
__________ |
2209 |
Transportation Invoice, (Single Sheet) |
__________ |
1444 |
Provider Invoice Envelope |
__________ |
2209CF Transportation Invoice, (Continuous Feed Format) |
__________ |
2244 |
Transportation Invoice |
__________ |
2210 |
Medical Equipment / Supplies Invoice, (Single Sheet) |
__________ |
2246 |
Health Agency Invoice |
__________ |
2210CF Medical Equipment / Supplies Invoice, (Cont. Feed Format) __________ |
2247 |
Medical Equipment Supplies |
__________ |
2211 |
Laboratory / Portable X-Ray Invoice, (Single Sheet) |
__________ |
2248 |
NIPS Special Invoice Handling |
__________ |
2211CF Laboratory / Portable X-Ray Invoice, (Cont. Feed Format) |
__________ |
2294 |
Equip/Supplies Prior Approval |
__________ |
2212 |
Health Agency Invoice, (Single Sheet) |
__________ |
2300 |
Prior Approval Request |
__________ |
2212CF Health Agency Invoice, (Continuous Feed Format) |
__________ |
Additional Forms Needed, Not Listed Above: |
2360 |
Health Insurance Claim Form, (Single Sheet) |
__________ |
__________________________ |
__________ |
2360CF Health Insurance Claim Form, (Continuous Feed Format) |
__________ |
__________________________ |
__________ |
3797 |
Medicare Crossover Invoice (Single Sheet) |
__________ |
__________________________ |
__________ |
3797CF Medicare Crossover Invoice, (Continuous Feed Format) |
__________ |
__________________________ |
__________ |
Submit this form by fax or mail to the address listed above.
HFS 1517 (R-9-10) |
IL478-1023 |