
Any time you would like to fill out cdph application, you don't have to download any software - just try using our online PDF editor. The tool is consistently upgraded by our staff, acquiring additional functions and growing to be better. Here is what you would have to do to get going:
Step 1: Just click the "Get Form Button" in the top section of this page to get into our form editing tool. Here you will find all that is required to work with your file.
Step 2: This editor will give you the capability to change nearly all PDF documents in various ways. Transform it by adding customized text, adjust original content, and include a signature - all readily available!
This document will need you to provide some specific details; in order to ensure correctness, take the time to heed the recommendations directly below:
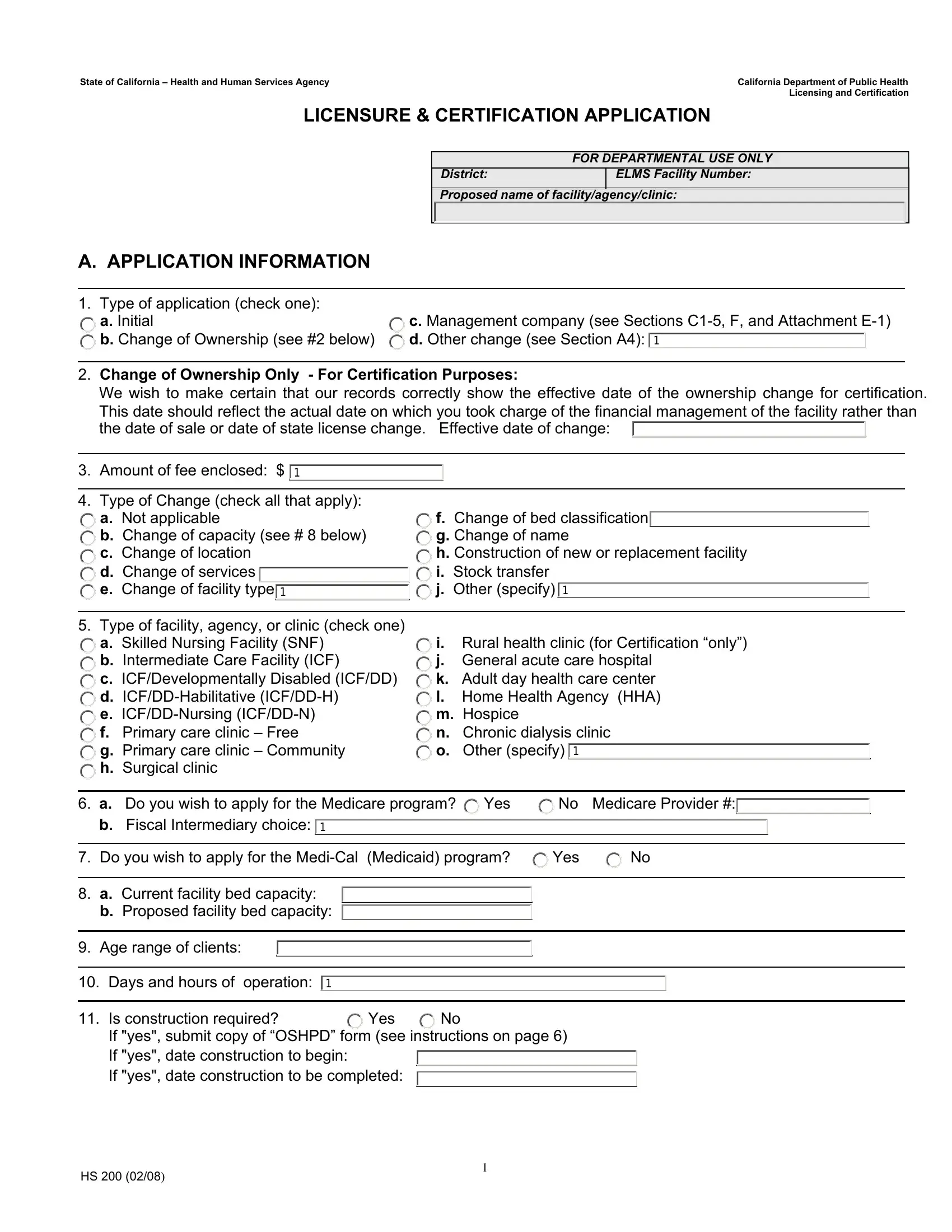
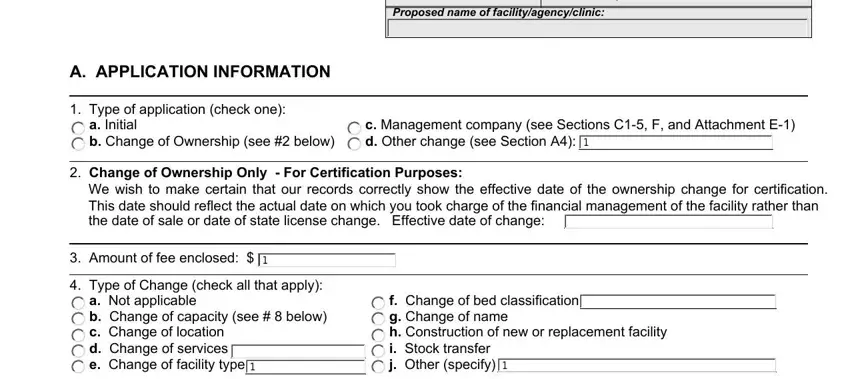
1. Firstly, once filling in the cdph application, start out with the part that includes the subsequent fields:
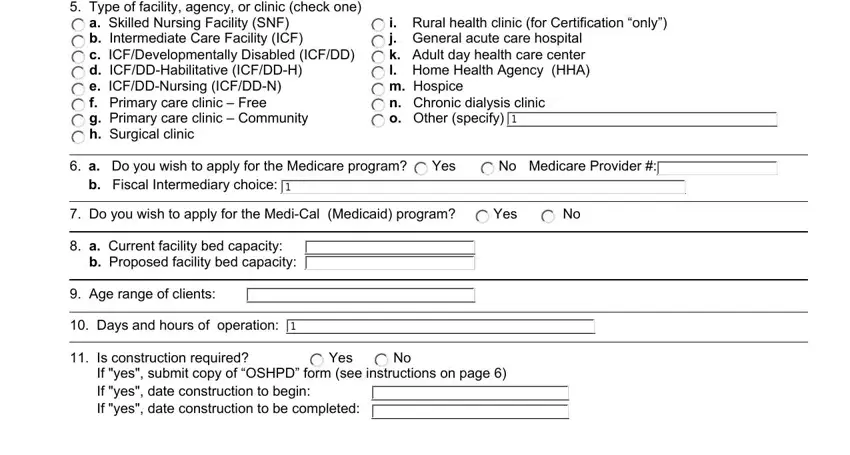
2. Just after performing the previous step, go to the subsequent step and fill in all required details in these fields - Type of facility agency or clinic, a Skilled Nursing Facility SNF b, i Rural health clinic for, a Do you wish to apply for the, Yes, Medicare Provider, b Fiscal Intermediary choice, Do you wish to apply for the, Yes, a Current facility bed capacity b, Age range of clients, Days and hours of operation, Is construction required, Yes, and If yes submit copy of OSHPD form.
3. The next part will be simple - fill out all the form fields in B LICENSEE INFORMATION, Licensee name, Federal employers tax ID number, Owner type check one Submit, a Sole proprietorship Individual b, g City h County i State agency j, Licensee address number street, Telephone number, City State Zip, EMail, Fax number, Identify other facilities agencies, Facility Name, Facility Type, and Facility address number street in order to complete this part.
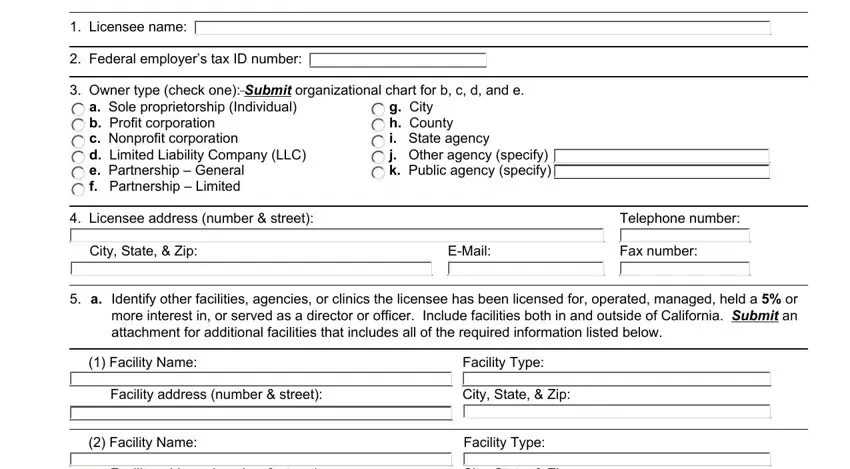
4. The following subsection requires your details in the subsequent places: Facility address number street, City State Zip, Facility Name, Facility Type, Facility address number street, City State Zip, Facility Name, Facility Type, Facility address number street, City State Zip, If any facility agency or clinic, Is the licensee a subsidiary of, Yes, If yes complete the information, and Parent organization name. Remember to provide all required info to go forward.
It's easy to make errors when completing the Facility Type, and so make sure you take a second look before you'll finalize the form.
5. This last section to conclude this form is pivotal. You need to fill in the required blank fields, such as Management Agreement this only, between the proposed owner and a, b Is there an interim management, owner to run the facility agency, Yes, Yes, Name of proposed facility agency, Current facility agency or clinic, Facility license number, Address number street of, Telephone number, City State Zip, Mailing address if different from, Telephone number, and Number Street, prior to using the form. Otherwise, it might produce an unfinished and possibly nonvalid paper!
Step 3: Ensure that the information is right and simply click "Done" to progress further. Sign up with us today and instantly access cdph application, available for downloading. Every last edit made is conveniently saved , which enables you to modify the pdf at a later stage if necessary. We do not sell or share the information that you provide while filling out forms at FormsPal.