Semi-Annual Performance Report
Multifamily Housing
Service Coordinator Program
U.S. Department of Housing |
OMB Approval |
and Urban Development |
No.2502-0447 |
Office of Housing |
(exp. 11/30/2016) |
Federal Housing Commissioner |
|
Public reporting burden for this collection of information is estimated to average 4 hours per response, including the time f or reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. This agency may not collect this information and you are not required to complete this form, unless it displays a currently valid control number.
Instructions: See pages 3 - 5 for detailed instructions.
|
1. R eporting Period |
2. Service Coordinator Information |
|
|
Oct. 1 |
- Mar 1, 20___ |
Name: |
Email address: |
|
Phone w/ area code: |
Number of weekly hrs at project: |
|
Apr. 1 |
- Sept. 30, 20___ |
|
|
|
|
|
|
Hire date: _____/_____/__________ |
|
3.S ource of funds for S ervice Coordinator
Debt Service Savings
Grant Provider #
4.Project Information
Project Name
Street Name, City, S tate, and Zip code
(check all that apply)
Residual Receipts
Section 236 Excess Income
Project Rental Assistance Project (PRAC)
Section 8 Operating Funds
# of Units |
# of Residents |
__
5. People S erved
a.R esident Age R anges
|
|
Age 1861 (i.e., nonelderly people w/disabilities) |
Age 6280 |
Age 8195 |
Over 96 |
Total |
|
|
|
|
|
b. R esidents' Functional S tatus |
|
|
Number SC Assisted During |
|
Type |
Number of Project Residents |
|
% of Total |
Reporting Period |
|
Frail Elders
At Risk Elders
Non-elders
All others
Total
c.Neighbors S erved
Number of lowincome elderly or people with disabilites who live in the neighborhood and whom you assisted during the reporting the period.
d. First Timers
Number of individuals whom you assisted for the first time during this reporting period.
New move ins |
Neighborhood residents |
All other project residents
Page 1 of 7 |
Form HUD 92456 2/2014 |
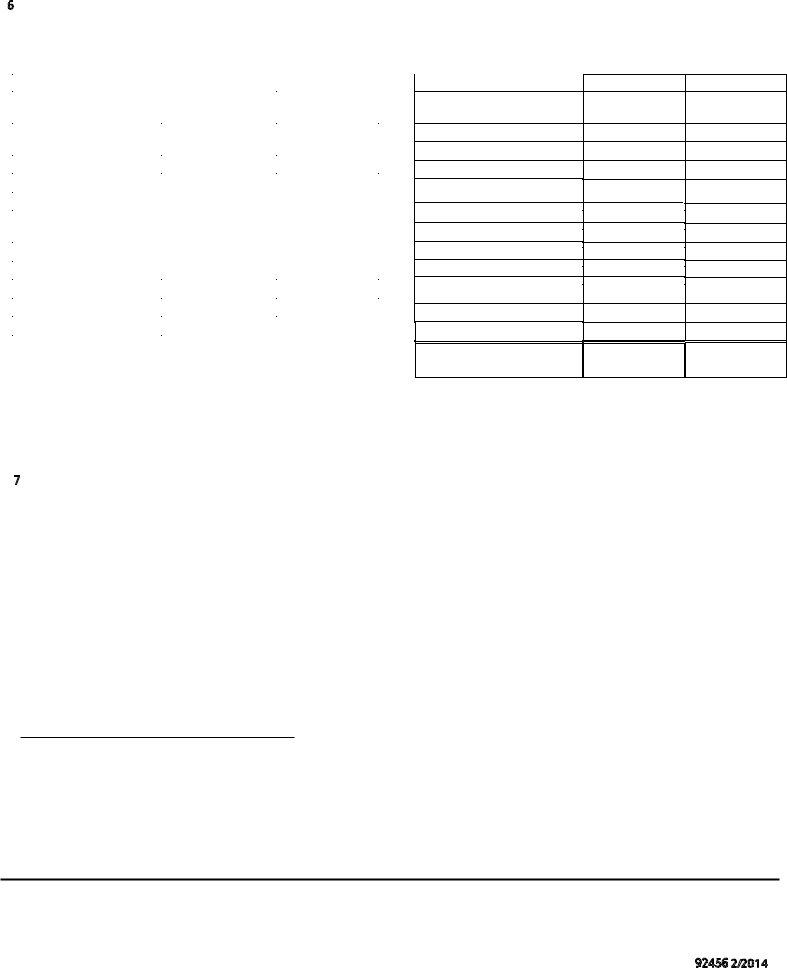
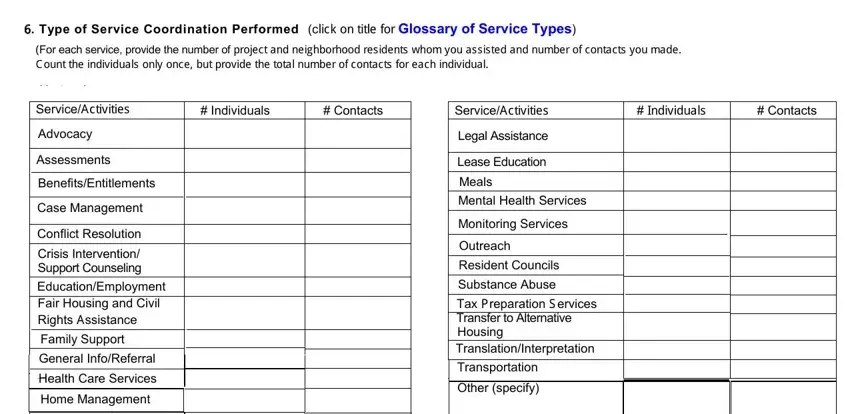
6. Type of Service Coordination Performed (click on title for Glossary of Service Types)
(For each service, provide the number of project and neighborhood residents whom you assisted and number of contacts you made.
Count the individuals only once, but provide the total number of contacts for each individual.
Service/Activities |
# Individuals |
# Contacts |
Advocacy |
|
|
|
|
|
Assessments |
|
|
|
|
|
Benefits/Entitlements |
|
|
|
|
|
Case Management |
|
|
|
|
|
Conflict Resolution |
|
|
|
|
|
Crisis Intervention/ |
|
|
Support Counseling |
|
|
|
|
|
Education/Employment |
|
|
|
|
|
Fair Housing and Civil |
|
|
Rights Assistance |
|
|
|
|
|
|
|
Family Support |
|
|
|
|
|
|
General Info/Referral |
|
|
|
|
|
|
|
Health Care Services |
|
|
|
|
|
Home Management |
|
|
|
|
|
Homemaker |
|
|
|
|
|
Isolation Intervention |
|
|
|
|
|
Service/Activities |
# Individuals |
# Contacts |
Legal Assistance
Lease Education
Meals
Mental Health Services
Monitoring Services
Outreach
Resident Councils
Substance Abuse
Tax Preparation S ervices
Transfer to Alternative
Housing
Translation/Interpretation
Transportation
Other (specify)
7. Aging in Place Statistics for Residents Who Moved Out of the Project During the R eporting Period.
Move-Out Reasons |
This Reporting Period |
Last Reporting Period |
|
Number of residents who died
Number of residents who moved to a higher level of care
Number of residents who moved in with family
Number of residents evicted
Other
Total number of move-outs
Page 2 of 7 |
Form HUD 92456 2/2014 |
8. Time Allocation of Monthly Tasks (List approximate % of time per month you performed these tasks. S um of all should equal 100%)
Contact with outside service providers |
% |
|
Paperwork not related to residents |
% |
|
|
|
Direct contact with project and neighborhood residents |
% |
Researching available services |
% |
|
Documentation of resident files |
% |
|
|
% |
|
|
Meetings with property management staff |
|
|
|
|
Other |
% |
|
|
|
|
|
|
Total 100% |
% |
|
Please respond to the following items 914 by attaching |
additional pages . |
|
|
9. Professional Training Duration (hours or days )
List the training programs you attended during this reporting period. Provide the name of the training provider and program, its location, number of hours, and the number of continuing education hours earned.
10. Educational / Preventative Health Programs
List the programs you implemented for project and/or neighborhood residents during this reporting period.
11. Fundraising
Fundraising activities are optional, but if you have engaged in any activities during the reporting period, please list them.
12. Community Engagement
List meetings or visits with community partners and attendance at or planning of community events that encourage interaction between the
community and project residents.
13. Resident Problems / Issues
Provide anecdotes (no more than two paragraphs each) describing two resident issues with which you were involved during this reporting period.
14. Additional Information
Provide any other information relevant to the administration and performance of the Service Coordinator Program. Provide any recommended "Best Practices" you have found to be effective in providing service coordination and promoting independent living for residents.
Service Coordinator's Name |
Date |
Page 3 of 7 |
Form HUD 92456 2/2014 |
Instructions for Completing Form HUD-92456General:
S ervice Coordinators whose positions are paid by any of the funding sources listed in item #3 must submit this
R eport. S ervice Coordinators must fill out the form; respond to all questions on the report, provide their name and the date the report is completed at the end of the form.
Multiple S ervice Coordinators, Projects, and Grants
*If one project has multiple Service Coordinators, each Service Coordinator should submit his/her own report.
*If one Service Coordinator serves multiple projects, submit one report per project. Y ou may submit one form per project, providing data for items1 through 8. Y ou may attach just one text document responding to items 9 through 14.
*If one Service Coordinator position is supported by two or more grants at one project, submit one report and include all grant numbers in item 3.
*If a Service Coordinator leaves his/her job during a reporting period, he or she must, to the extent possible, complete a performance report for the time worked during that reporting period. If a new S ervice Coordinator starts during the same reporting period, he or she should similarly complete a report for the time worked during that reporting period. The S ervice Coordinator who finishes out the reporting period must send both reports to HUD, to provide data for the entire reporting period.
Method of S ubmission
It is preferred that you complete items 1 through 8 on the form on your computer and create a text file that contains brief responses to items 9 through 14. Email both files together in one email to your representative in the HUD field office that services your project. If you are unable to create or email electronic files, you may complete and submit a hard paper copy to your local HUD representative.
S pecific Instructions for E ach Item:
1.R eporting Period: All Service Coordinators must submit this Report according to the Federal Fiscal Year dates. The reporting periods are October 1 through March 31 and April 1 through September 30. Your Report is due to your local Field Office 30 days after the end of the reporting period, i.e. April 30 and October 30, respectively. Fill in the two-digit year on March 31 or September 30.
2.S ervice Coordinator's Information. Enter your name, phone number, and email address. Provide the month and year you started in this position. Indicate the number of hours you work each week at the project listed in item #4.
3. S ource of Funds for the S ervice Coordinator.
Indicate all sources of HUD funding that are used to pay for your position. Many projects do use a combination of sources.
*If your position is supported by a HUD grant, check the "Grant" box and provide the grant number(s). The middle four digits of this number must begin with: "C93", "C94", "CS", OR "HS". An example is OK56HS02002.
Do not provide your project's Section 8 number (e.g. OK56H789021).
*Check "Debt S ervice S avings", "R esidual R eceipts", or "S ection 236 E xcess Income if your local HUD office has approved the use of thses funds for the S ervice Coordinator program.
*Check "S ection 8 or S ection 202 PR AC operating funds" if your local HUD office has approved the S ervice Coordinator as an ongoing permanent expense in your project's operating budget.
*Check multiple boxes if you use two or more HUD sources of funds to pay for your program. For example, many programs are supported by a combination of grant funds and residual receipts or grant funds and S ection 8 funds.
4.Project Information. Provide the name and address of the property where you work. Give the total number of units (i.e. apartments) in the project and the total number of residents. R emember that if you serve two or more projects you must complete a separate report for each project.
5.People S erved
5a. R esident Age R anges. Provide number of residents in each age category. The total of the four categories should match the number of residents provided in item #4.
5b. R esidents' Functional S tatus. Provide the estimated number of frail, atrisk, and well elderly (aged 62+) and the number of nonelderly people with disabilities. (aged 1861). The "All others" line refers to the "well" elderly.
Indicate the number of residents in each category whom you assisted in any way during the reporting period. Do not count residents twice. R egardless of the amount of time spent assisting one resident, only count that individual once. The total of the four categories in the "Number of Project R esidents" column should match the number of residents provided in item #4.
A "Frail" elder is someone who has difficulty performing three or more Activities of Daily Living (ADLs). An "Atrisk" elder is one who has difficulty performing one or two ADLs. ADL deficiencies do not appy to nonelderly people with disabilities.
Page 4 of 7 |
Form HUD 92456 2/2014 |
HUD's definition of ADLs includes eating, dressing, bathing, grooming, and transferring, as further described below:
(1)Eating--may need assistance with cooking, preparing, or serving food, but must be able to feed self;
(2)Bathing--may need assistance in getting in and out of the shower or tub, but must be able to wash self;
(3)Grooming--may need assistance in washing hair, but must be able to take care of personal appearance;
(4)Dressing--must be able to dress self, but may need occasional assistance;
(5)Transferring---actions such as going from a seated to standing position, getting in and out of bed, and using the toilet.
5c. Neighbors S erved. Provide the number of low-income elderly or people with disabilities who live in the neighborhood whom you assisted during the reporting period (if any). Working with neighborhood residents is optional. HUD is interested in knowing how many S ervice Coordinators serve the greater community and how many individuals are covered.
5d. First Timers. Provide the number of project residents and neighbors whom you assisted for the first time during the reporting period.
Make a distinction between those who moved in within the last six months ("New move-ins") and those who have lived in the project or neighborhood longer, but only started coming to you for assistance during this reporting period.
6.Type of S ervice Coordination Performed. For each of the listed services, provide the sum of project residents and neighbors (in the "Number of Individuals" column) who received that service during the reporting period. Provide the number of contacts
with all individuals related to those services. Choose only the category you feel most appropriately represents the service you coordinated.
Count individuals once but report each contact with that one person. For example, you assisted three project residents in obtaining transportation services during the reporting period. To do this you had to meet with one resident three times, another resident five times and the third resident three times. S o the number of individuals is three and the number of contacts is 11.
If you additionally helped one neighborhood resident obtain transportation services and if you met with that person three times during the reporting period, then the number of individuals will be 4 and the number of contacts will be 14. R efer to the Glossary of S ervice Types (HUD92456G) for explanations and examples of services.
7. Aging in Place S tatistics. Provide the number of project residents who left the project during the reporting period.
Residents counted in this section must have been residents of the project at the time of their departure. Do not count neighborhood residents. Provide the reason and number for each move-out. Add other reasons on the "Other" line if relevant.
HUD wants to know how the Service Coordinator program affects aging-in-place over time. Include the numbers from the last report as a comparison. You'll do this on each subsequent report. If you are a new S ervice Coordinator and don't have a previous report or access to previous data, indicate "No Data" in the revelant box.
8. Time Allocation of Monthly Tasks. List the approximate or average % of time per month you spent performing the listed tasks. Add others if appropriate. Sum of all should equal 100% of your average time each month.
*Contact with outside service providers. Includes any activity related to obtaining information about or advocating for affordable supportive services or assistance for residents. Such activity may include telephone conversations, face-to-face meetings, coalition or task force meetings, or working groups.
*Direct contact with project and neighborhood residents. This is the time you spend with your residents, for example in oneonone meetings, informal conversation, while conducting needs screenings, or at educational program gatherings.
Page 5 of 7 |
Form HUD 92456 |
2/2014 |
|
|
*Documentation of resident files. Includes any notes you make, forms completed, or other information entered in resident files.
*M eetings with property management staff. Includes meetings with site manager or administrator, supervisor, other property management staff, or any other related meeting.
*Paperwork not related to a resident. Includes any reports written for management staff, supervisors, or peers.
Also relevant is paperwork related to registering for training, arranging travel, or purchasing supplies or equipment.
*Researching available services. Includes time spent searching for program information on the Internet, by phone, reading literature, and meeting with knowledgeable professionals.
*O ther. If you perform other work on a monthly basis, please list function and percentage of time.
Please attach a Microsoft Word (or other text file) that contains brief responses to items 9-14. Your report is not
complete without this additional document and adequate responses to each item.
9. Professional raining Duration (hours or days) |
.*List the eligible training programs you attended during this |
reporting period. Provide the following information for each program you attended:
*Name of the training program
*Name of sponsoring organization that planned and executed the training ( i.e. training provider)
*Location
*Duration ( hours or days)
*Number of training hours completed
* Training pursuant to guidance in HUD' s M anagement Agent Handbook4381 .5 REV 2 CHG 2, Chapter 8.9. First time S ervice Coordinators must complete 36 hours in the first year of employment as a S ervice Coordinator, unless they have received recent revelant training. All other S ervice Coordinators must complete 12 hours of eligible training each year.
10.Educational and Preventative Health Pro grams. List the programs you developed and/or implemented for project and/or neighborhood residents during this reporting period. Provide the name or topic of each program only and give the approximate number of individuals who attended. Indicate whether events were one time only or ongoing programs.
Examples of such programs are talks on osteoporosis, nutrition, or accessibility issues for people with disabilities, “brown bag” medication meetings with pharmacists, or remembrance groups.
Page 6 of 7 |
Form HUD 9245 62 2 14 |
11. Fundraising. List optional fundraising activities, if any, completed during this reporting period. Provide the name
or brief description of each activity, the amount of funds raised, and the intended use of these funds. Please note that fundraising activities must relate to assisting the residents to age in place.
Examples of items that you might assist in fundraising include but are not limited to:
Another part-time Service Coordinator or aide position
Exercise equipment
Blood pressure machine for health clinic use
Ramp to make the project or immediate area more accessible
Purchase or lease of a van
Creation of computer Center and purchase of computer equipment
Examples of items that you should not directly engage in fundraising activities for include:
Holiday parties
Large screen TVs for community rooms
DVD players
Pianos and organs
Bingo sets
12. Community Engagement. List meetings with service providers and local area partners and attendance at or planning of local events that encourage interaction between the greater community and project residents.
Community engagement is defined as follows:
*Visits or meetings with new service providers and/or local vendors, churches, schools, etc.
*Attendance at community organization events that would make the greater community aware of your property and the needs of your residents.
*Planning events that encourage the greater community to visit and interact with project residents.
13. Resident Problems/Issues. Provide anecdotes (no more than two paragraphs each) describing two resident issues with which you were involved during the reporting period. Indicate whether or not the issue was resolved during the
reporting period. Describe positive and/or negative outcomes. The objective of this item is to give readers of the report
a description of your work and the types of issues dealt with on a daily basis. Unresolved situations will be viewed as
examples of difficult problems or circumstances and not as a negative reflection on your efforts. Please be candid in your account, in order to give the reader an accurate description of your work. Do not provide any personal identifiable
information.
14.Additional Information. Provide any other information relevant to the administration and performance of the Service Coordinator Program. Provide any recommended "Best Practices" you have found to be effective in providing service
coordination and promoting independent living for the residents. Examples of your "Best Practices" will be essential in helping others develop effective S ervice Coordinator programs and obtaining needed resources.
Page 7 of 7 |
Form HUD 92456 2/2014 |