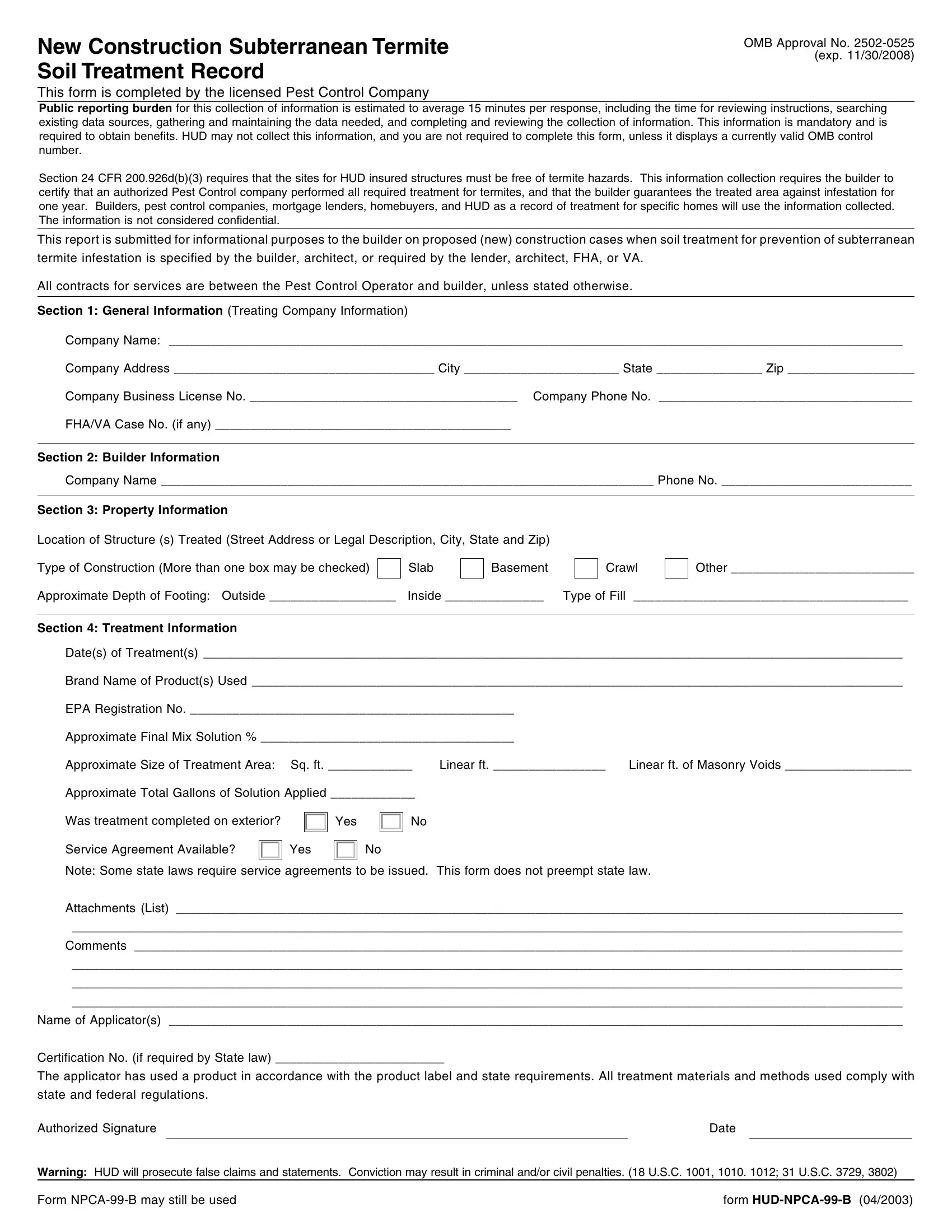
New Construction Subterranean Termite Soil Treatment Record
OMB Approval No. 2502-0525 (exp. 11/30/2008)
This form is completed by the licensed Pest Control Company
Public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. This information is mandatory and is required to obtain benefits. HUD may not collect this information, and you are not required to complete this form, unless it displays a currently valid OMB control number.
Section 24 CFR 200.926d(b)(3) requires that the sites for HUD insured structures must be free of termite hazards. This information collection requires the builder to certify that an authorized Pest Control company performed all required treatment for termites, and that the builder guarantees the treated area against infestation for one year. Builders, pest control companies, mortgage lenders, homebuyers, and HUD as a record of treatment for specific homes will use the information collected. The information is not considered confidential.
This report is submitted for informational purposes to the builder on proposed (new) construction cases when soil treatment for prevention of subterranean termite infestation is specified by the builder, architect, or required by the lender, architect, FHA, or VA.
All contracts for services are between the Pest Control Operator and builder, unless stated otherwise.
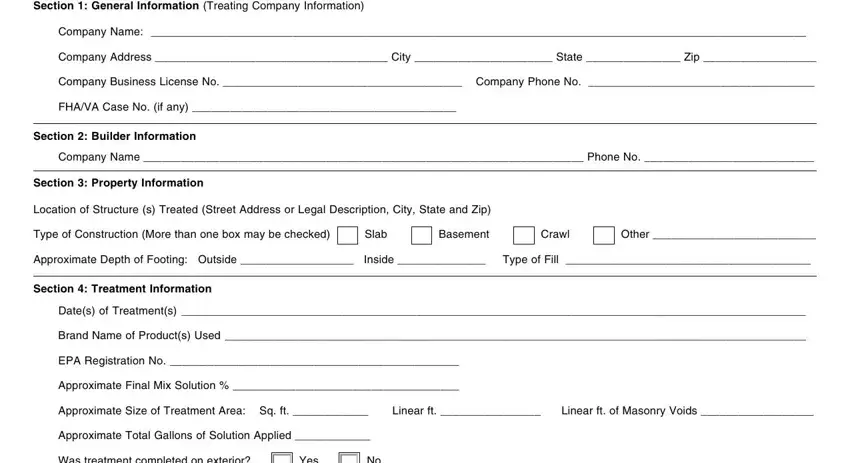
Section 1: General Information (Treating Company Information)
Company Name: __________________________________________________________________________________________________________
Company Address _____________________________________ City ______________________ State _______________ Zip __________________
Company Business License No. ______________________________________ Company Phone No. ____________________________________
FHA/VA Case No. (if any) __________________________________________
Section 2: Builder Information
Company Name ______________________________________________________________________ Phone No. ___________________________
Section 3: Property Information
Location of Structure (s) Treated (Street Address or Legal Description, City, State and Zip)
Type of Construction (More than one box may be checked)
Other __________________________
Approximate Depth of Footing: Outside __________________ Inside ______________ Type of Fill _______________________________________
Section 4: Treatment Information
Date(s) of Treatment(s) _____________________________________________________________________________________________________
Brand Name of Product(s) Used ______________________________________________________________________________________________
EPA Registration No. ______________________________________________ |
|
Approximate Final Mix Solution % ____________________________________ |
|
Approximate Size of Treatment Area: Sq. ft. ____________ |
Linear ft. ________________ |
Linear ft. of Masonry Voids __________________ |
Approximate Total Gallons of Solution Applied ____________ |
|
|
Was treatment completed on exterior?
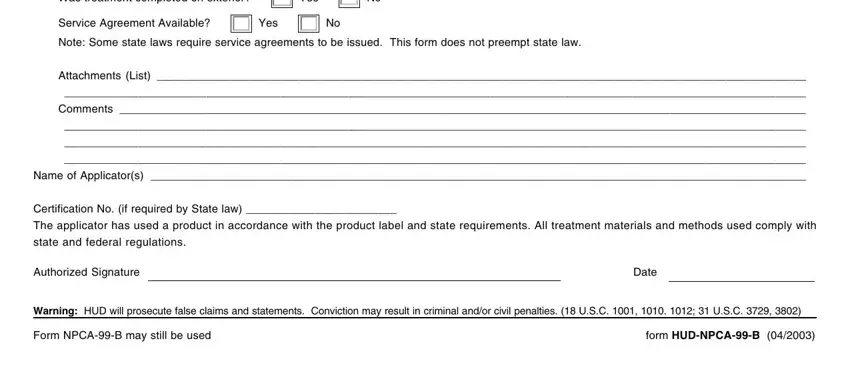
Service Agreement Available?
Note: Some state laws require service agreements to be issued. This form does not preempt state law.
Attachments (List) _________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
Comments _______________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
Name of Applicator(s) __________________________________________________________________________________________________________
Certification No. (if required by State law) ________________________
The applicator has used a product in accordance with the product label and state requirements. All treatment materials and methods used comply with state and federal regulations.
Authorized SignatureDate
Warning: HUD will prosecute false claims and statements. Conviction may result in criminal and/or civil penalties. (18 U.S.C. 1001, 1010. 1012; 31 U.S.C. 3729, 3802)
Form NPCA-99-B may still be used |
form HUD-NPCA-99-B (04/2003) |