

Whenever you would like to fill out ihs release of information form, there's no need to download any sort of applications - simply try using our online PDF editor. Our editor is continually developing to give the very best user experience achievable, and that is thanks to our resolve for continuous improvement and listening closely to feedback from users. This is what you would have to do to get going:
Step 1: Just press the "Get Form Button" above on this page to start up our pdf form editing tool. This way, you'll find everything that is necessary to fill out your document.
Step 2: As you start the editor, you'll notice the document prepared to be filled in. In addition to filling in various fields, you could also do some other actions with the file, particularly writing your own words, changing the initial text, adding illustrations or photos, putting your signature on the document, and more.
It really is easy to complete the form with this detailed guide! Here's what you need to do:
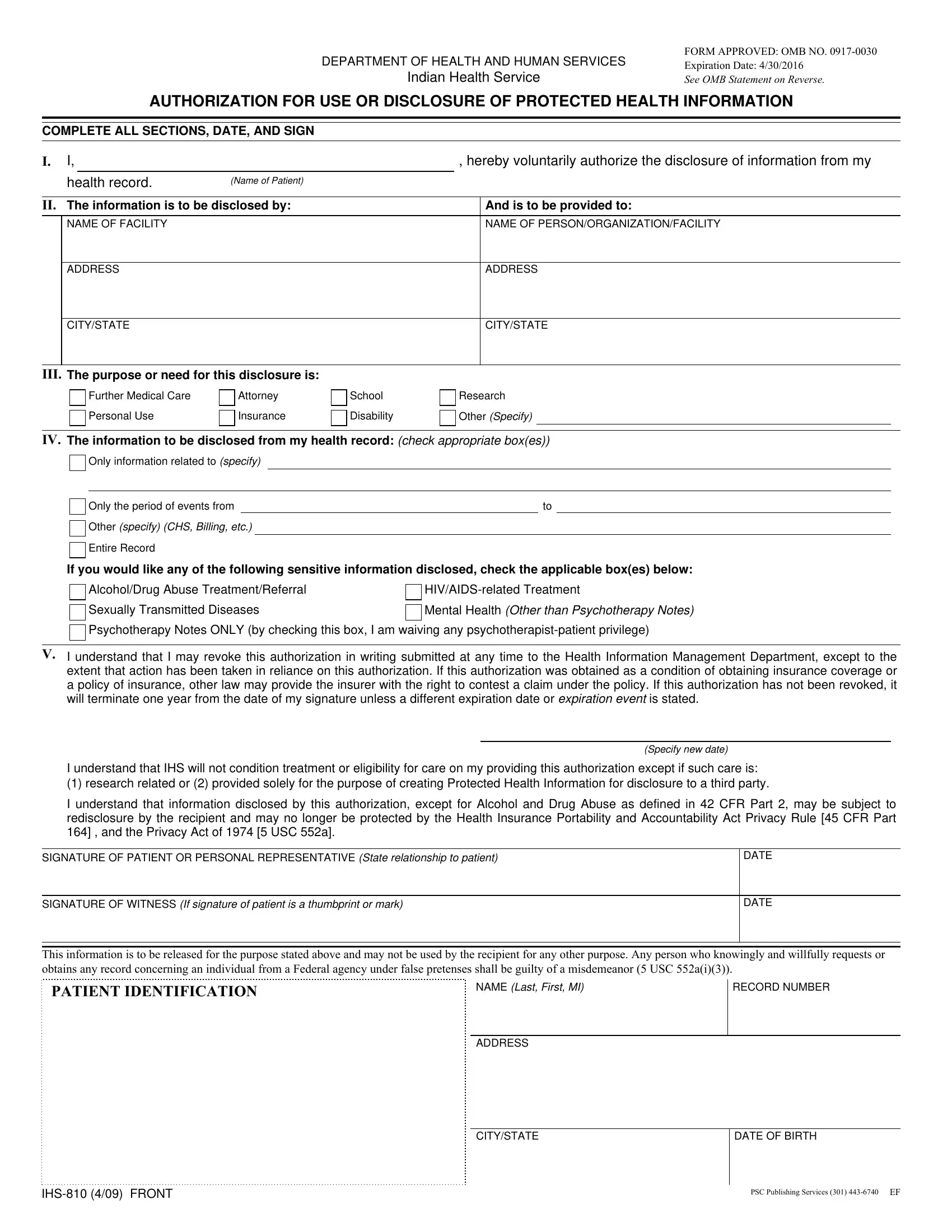
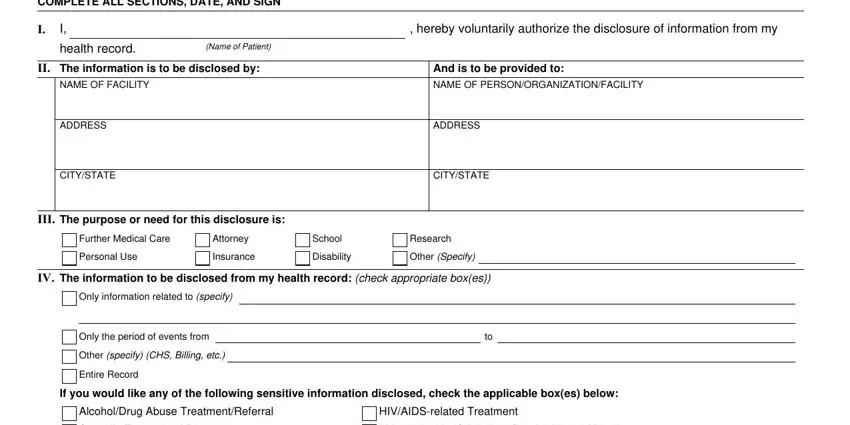
1. When completing the ihs release of information form, make certain to incorporate all essential blanks within its corresponding section. This will help to facilitate the work, allowing for your information to be processed fast and correctly.
2. The subsequent stage is usually to fill out these particular blanks: Sexually Transmitted Diseases, Mental Health Other than, Psychotherapy Notes ONLY by, I understand that I may revoke, I understand that IHS will not, I understand that information, Specify new date, SIGNATURE OF PATIENT OR PERSONAL, SIGNATURE OF WITNESS If signature, DATE, DATE, This information is to be released, NAME Last First MI, and RECORD NUMBER.
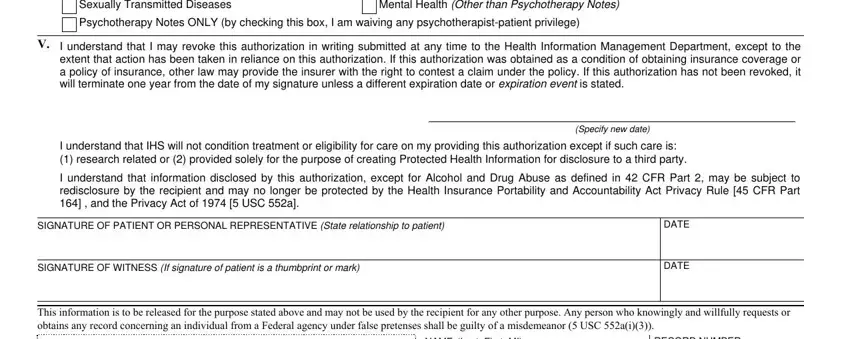
3. Completing PATIENT IDENTIFICATION, NAME Last First MI, RECORD NUMBER, ADDRESS, CITYSTATE, DATE OF BIRTH, IHS FRONT, and PSC Publishing Services EF is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
It is possible to get it wrong when completing your DATE OF BIRTH, for that reason be sure you reread it before you send it in.
Step 3: Prior to moving on, ensure that blanks were filled in correctly. When you believe it is all good, click on “Done." Join FormsPal today and easily get access to ihs release of information form, all set for download. All changes made by you are preserved , making it possible to modify the pdf later on if required. At FormsPal.com, we strive to be sure that your information is kept secure.