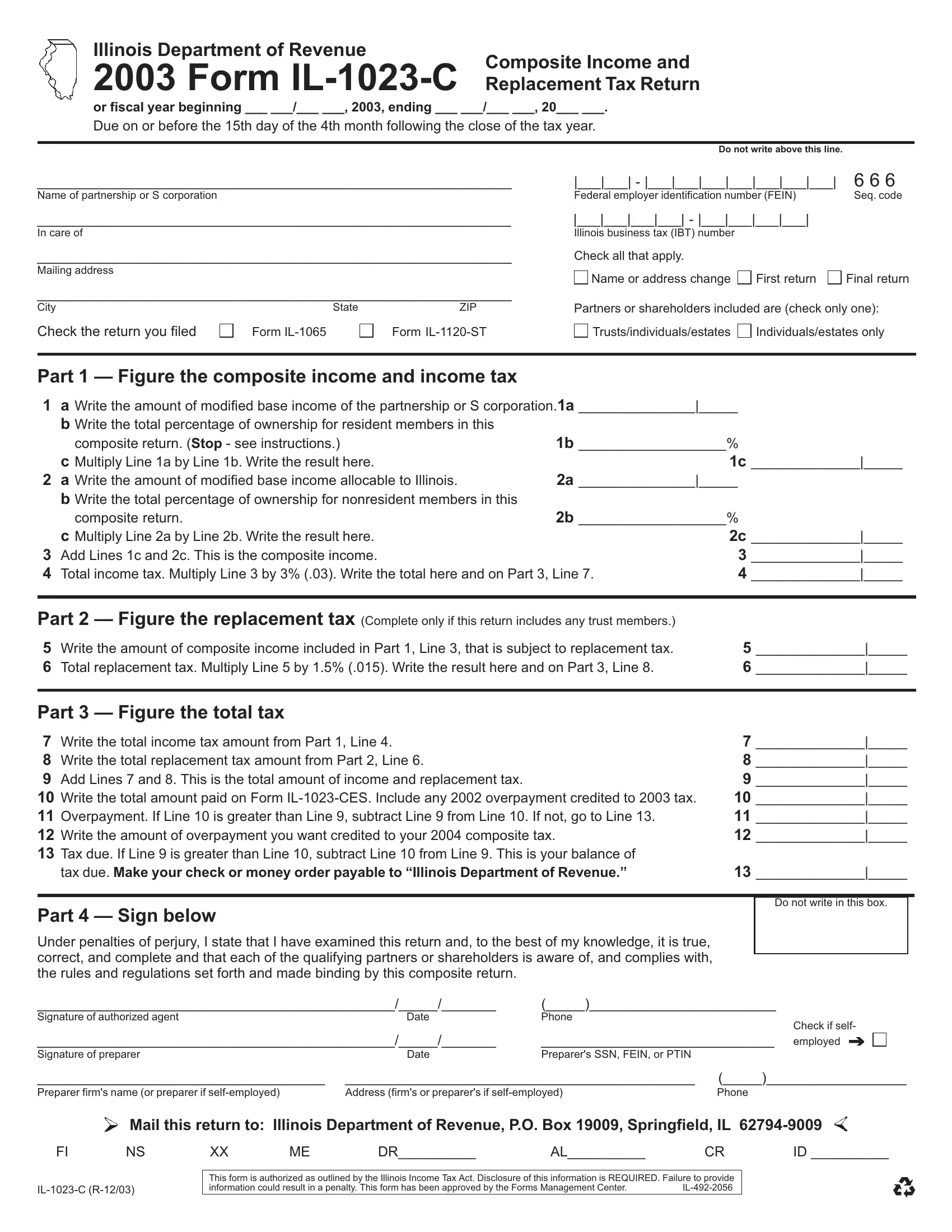
Navigating the complexities of state taxation can often feel like interpreting an intricate code made up of forms, figures, and deadlines. Among these, the Illinois Department of Revenue's Form IL-1023-C stands out for partnerships and S corporations engaged in filing a Composite Income and Replacement Tax Return. Designed for the fiscal year starting in 2003, this form serves as a critical tool for entities opting to file a combined return on behalf of their nonresident members, simplifying the tax filing process and compliance with state tax obligations. The form meticulously guides filers through calculating the modified base income, apportioning income between resident and nonresident members, and determining the total income and replacement taxes due. It demands careful attention to percentages of ownership and allocable income to Illinois. Furthermore, the form allows for the designation of changes, such as a change in name or address, the marking of the return as the first or final filing, and the inclusion of trusts, individuals, or estates. The detailed instructions endeavor to ensure accurate reporting and to facilitate the calculation of taxes due or overpayments, ultimately culminating in the precise balance of tax payable to the Illinois Department of Revenue. As taxing as it might appear at first glance, Form IL-1023-C embodies the state's effort to streamline tax reporting and payment for composite filers, framing a clearer path through the often-thorny thicket of tax compliance.
| Question | Answer |
|---|---|
| Form Name | Form Il 1023 C |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Illinois, nonresident, 15th, illinois department of revenue change of address |
Illinois Department of Revenue |
Composite Income and |
|
2003 Form |
||
ReplacementTaxReturn |
or fiscal year beginning ___ ___/___ ___, 2003, ending ___ ___/___ ___, 20___ ___.
Due on or before the 15th day of the 4th month following the close of the tax year.
Do not write above this line.
_____________________________________________________________ |
|___|___| - |___|___|___|___|___|___|___| |
6 6 6 |
|
Name of partnership or S corporation |
Federal employer identification number (FEIN) |
Seq.code |
|
_____________________________________________________________ |
|___|___|___|___| - |___|___|___|___| |
|
|
In care of |
Illinois business tax (IBT) number |
|
|
_____________________________________________________________ |
Check all that apply. |
|
|
Mailing address |
Name or address change |
First return |
Final return |
|
|||
_____________________________________________________________
City
Check the return you filed
State
Form
ZIP |
Partners or shareholders included are (check only one): |
|
Form |
Trusts/individuals/estates |
Individuals/estates only |
Part 1 — Figure the composite income and income tax
1a Write the amount of modified base income of the partnership or S corporation.1a _______________|_____
b Write the total percentage of ownership for resident members in this
|
composite return. (Stop - see instructions.) |
1b ___________________% |
|
|
|
|
c Multiply Line 1a by Line 1b. Write the result here. |
|
1c |
______________|_____ |
|
2 |
a Write the amount of modified base income allocable to Illinois. |
2a _______________|_____ |
|
|
|
|
b Write the total percentage of ownership for nonresident members in this |
|
|
|
|
|
composite return. |
2b ___________________% |
|
|
|
|
c Multiply Line 2a by Line 2b. Write the result here. |
|
2c |
______________|_____ |
|
3 |
Add Lines 1c and 2c. This is the composite income. |
|
3 |
______________|_____ |
|
4 |
Total income tax. Multiply Line 3 by 3% (.03). Write the total here and on Part 3, Line 7. |
4 |
______________|_____ |
||
|
|
|
|
||
Part 2 — Figure the replacement tax (Complete only if this return includes any trust members.) |
|
|
|
||
5 |
Write the amount of composite income included in Part 1, Line 3, that is subject to replacement tax. |
5 |
______________|_____ |
||
6 |
Total replacement tax. Multiply Line 5 by 1.5% (.015). Write the result here and on Part 3, Line 8. |
6 |
______________|_____ |
||
|
|
|
|
|
|
Part 3 — Figure the total tax |
|
|
|
|
|
7 |
Write the total income tax amount from Part 1, Line 4. |
|
7 |
______________|_____ |
|
8 |
Write the total replacement tax amount from Part 2, Line 6. |
|
8 |
______________|_____ |
|
9 |
Add Lines 7 and 8. This is the total amount of income and replacement tax. |
|
9 |
______________|_____ |
|
10 |
Write the total amount paid on Form |
10 |
______________|_____ |
||
11 |
Overpayment. If Line 10 is greater than Line 9, subtract Line 9 from Line 10. If not, go to Line 13. |
11 |
______________|_____ |
||
12 |
Write the amount of overpayment you want credited to your 2004 composite tax. |
|
12 |
______________|_____ |
|
13Tax due. If Line 9 is greater than Line 10, subtract Line 10 from Line 9. This is your balance of
taxdue.Makeyourcheckormoneyorderpayableto“IllinoisDepartmentofRevenue.” |
13 ______________|_____ |
Part 4 — Sign below
Under penalties of perjury, I state that I have examined this return and, to the best of my knowledge, it is true, correct, and complete and that each of the qualifying partners or shareholders is aware of, and complies with, the rules and regulations set forth and made binding by this composite return.
Do not write in this box.
______________________________________________/_____/_______ |
(_____)________________________ |
|
Signatureofauthorizedagent |
Date |
Phone |
|
|
Check if self- |
______________________________________________/_____/_______ |
______________________________ employed |
|
Signature of preparer |
Date |
Preparer's SSN, FEIN, or PTIN |
_____________________________________ _____________________________________________ (_____)__________________
Mail this return to: Illinois Department of Revenue, P.O. Box 19009, Springfield, IL
FI |
NS |
XX |
ME |
DR__________ |
AL__________ |
CR |
ID __________ |
This form is authorized as outlined by the Illinois Income Tax Act. Disclosure of this information is REQUIRED. Failure to provide
information could result in a penalty. This form has been approved by the Forms Management Center. |