
AHCA Form 3110 1023 can be completed online using the FormsPal PDF editor. The tool lets you fill in all required fields, add text, insert your signature, and save or print the completed document at no cost.
Step 1: First, access the pdf editor by pressing the "Get Form Button" in the top section of this webpage.
Step 2: Once you start the editor, you will find the document all set to be filled in. Apart from filling in various fields, it's also possible to perform other things with the Document, that is adding any textual content, changing the original textual content, adding graphics, placing your signature to the PDF, and much more.
Completing this document requires care for details. Make sure each field is done correctly.
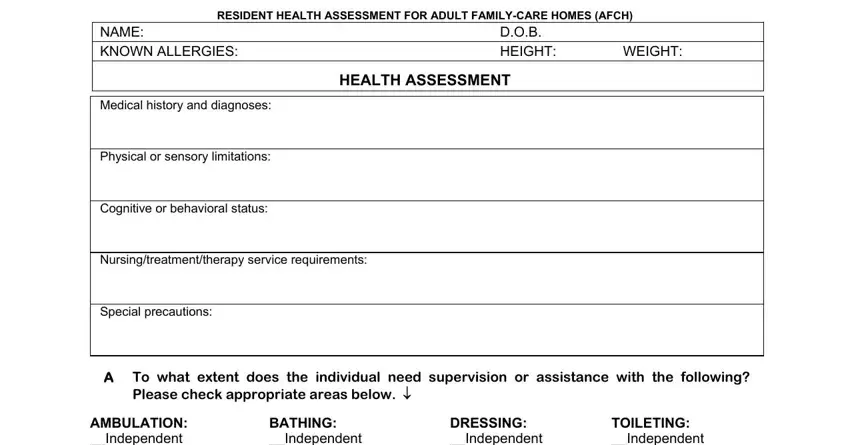
1. Start completing your AHCA Form 3110 1023 with a group of major blank fields. Gather all of the required information and ensure not a single thing overlooked!
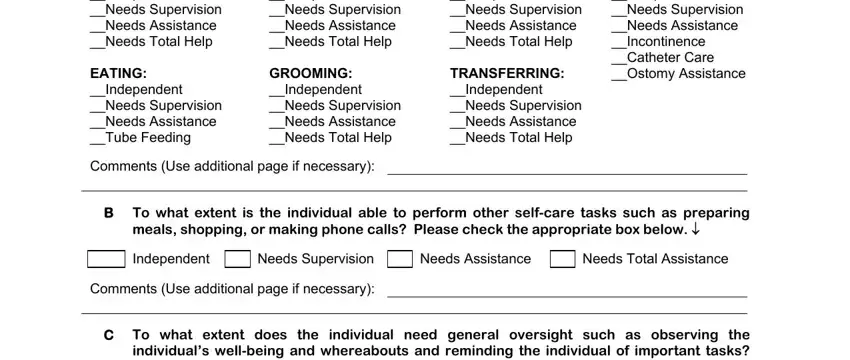
2. Right after completing this step, head on to the next step and fill in all required particulars in these fields - AMBULATION Independent Needs, BATHING Independent Needs, TOILETING Independent Needs, DRESSING Independent Needs, B To what extent is the individual, meals shopping or making phone, Independent, Needs Supervision, Comments Use additional page if, Needs Assistance, Needs Total Assistance, and C To what extent does the.
People often make errors when filling out AMBULATION Independent Needs in this section. Make sure you review everything you type in right here.
3. The following section focuses on C To what extent does the, Independent, Weekly Oversight, Daily Oversight, Other Please describe below, Comments Use additional page if, and AHCA Form AFCH Rule A FAC - fill in all these blanks.
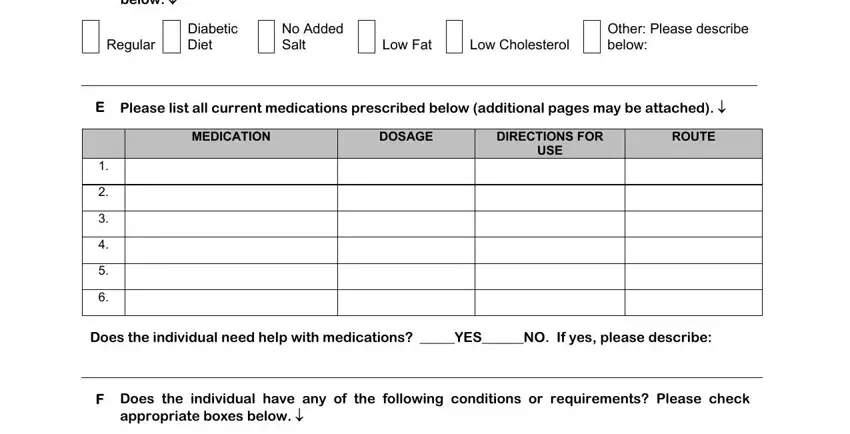
4. Completing below, Regular, Diabetic, No Added, Diet, Salt, Low Fat, Low Cholesterol, Other Please describe, below, E Please list all current, MEDICATION, DOSAGE, DIRECTIONS FOR, and ROUTE is essential in this fourth step - be certain to take the time and take a close look at every field!
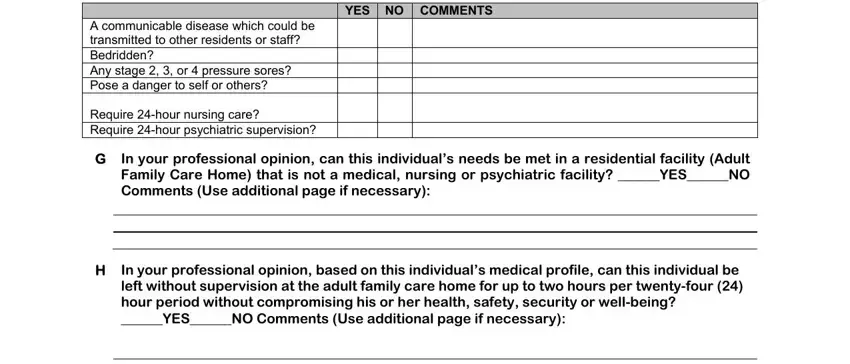
5. The final stage to finish this PDF form is pivotal. Make certain to fill in the necessary blanks, like A communicable disease which could, YES NO COMMENTS, In your professional opinion can, and In your professional opinion based, before using the file. Otherwise, it may result in an incomplete and possibly invalid document!
Step 3: Immediately after double-checking the form fields, hit "Done" and you are good to go! After creating a free account, it will be possible to download AHCA Form 3110 1023 or send it via email. The file will also be accessible via your personal cabinet with all modifications. We don't share or sell any information provided when filling out documents at our site.
Also useful: AHCA Form 1823 (ALF resident assessment), AHCA Form 3020, and the Nursing Home Form.