
varies can be completed online without difficulty. Simply make use of FormsPal PDF editor to finish the job without delay. Our tool is constantly developing to give the best user experience achievable, and that's thanks to our dedication to continuous enhancement and listening closely to customer feedback. Starting is simple! Everything you should do is adhere to the following basic steps down below:
Step 1: Click the "Get Form" button above on this webpage to access our PDF tool.
Step 2: After you access the online editor, you'll see the document made ready to be filled in. Apart from filling in different blank fields, you may as well do other sorts of things with the form, that is adding your own text, modifying the initial textual content, inserting graphics, affixing your signature to the form, and more.
This document will require particular data to be entered, hence be sure to take whatever time to type in precisely what is expected:
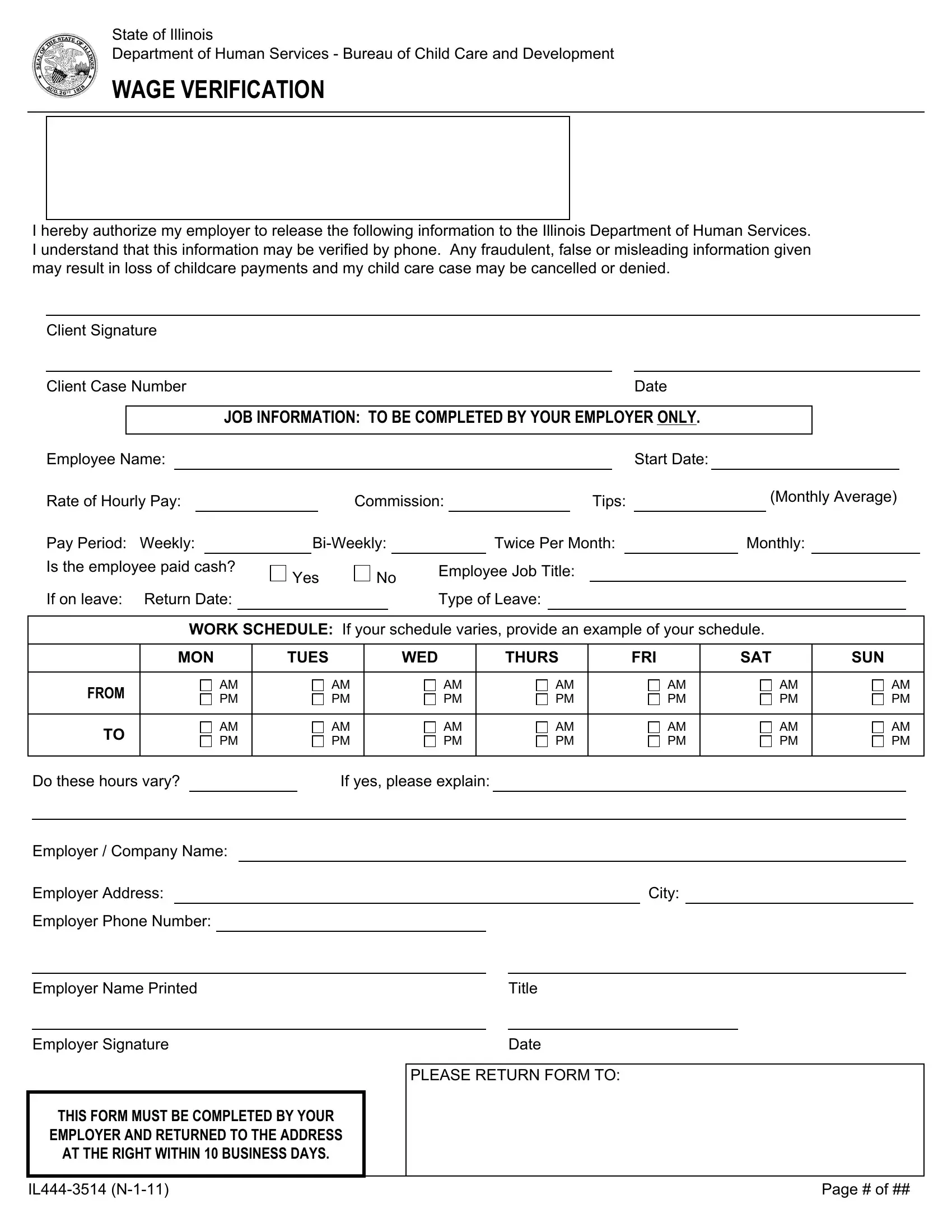
1. It is critical to fill out the varies properly, hence pay close attention while filling in the segments comprising these specific blanks:
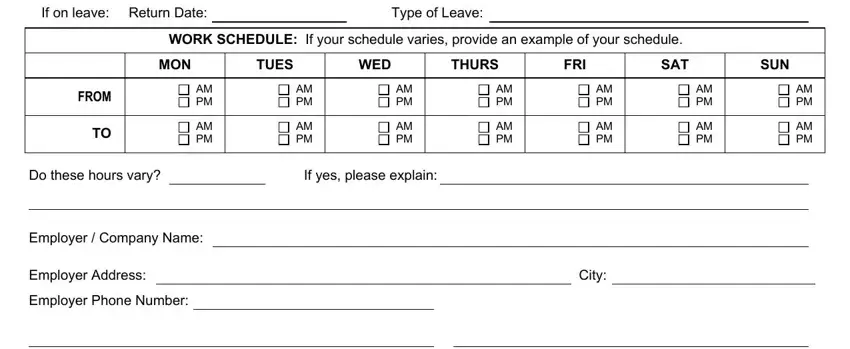
2. Once your current task is complete, take the next step – fill out all of these fields - If on leave Return Date, Yes, Type of Leave, WORK SCHEDULE If your schedule, MON, TUES, WED, THURS, FRI, SAT, SUN, FROM, AM PM, AM PM, and AM PM with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. In this specific stage, have a look at Employer Name Printed, Employer Signature, THIS FORM MUST BE COMPLETED BY YOUR, EMPLOYER AND RETURNED TO THE, AT THE RIGHT WITHIN BUSINESS DAYS, Title, Date, PLEASE RETURN FORM TO, IL N, and Page of. All of these have to be filled out with utmost focus on detail.
People who work with this form frequently make errors while filling out IL N in this part. Ensure you revise everything you enter here.
Step 3: As soon as you've reviewed the details in the file's blanks, just click "Done" to finalize your document creation. Join us today and easily use varies, all set for downloading. Each edit made is handily preserved , letting you edit the file later on when necessary. At FormsPal, we do our utmost to ensure that all of your details are stored private.