The Health Insurance Benefits Agreement, governed by the Department of Health and Human Services and specifically designed for Rural Health Clinics, is a fundamental document that establishes these clinics' eligibility for payment under Title XVIII of the Social Security Act. This meticulously structured agreement mandates adherence to the certification conditions outlined in part 491 of chapter IV, title 42 of the Code of Federal Regulations. It emphasizes the importance of transparency in reporting compliance failures to the Centers for Medicare & Medicaid Services. Additionally, it restricts clinics from billing beneficiaries for covered services except for approved deductible or coinsurance amounts and mandates prompt refunds of any incorrect charges. Ensuring equitable treatment of Medicare beneficiaries and adding provisions to enhance Medicare program administration are also critical components. Significantly, this agreement is not only binding upon the Rural Health Clinic and the Secretary of Health and Human Services once accepted but also includes stipulations regarding ownership transfer, highlighting automatic assignment to new owners while maintaining adherence to existing conditions and corrective plans. The document concludes with a legal notice against false statements under federal law, underscoring the seriousness of the agreement. This framework ensures that Rural Health Clinics operate within a structured legal and ethical boundary, contributing to the efficient and effective administration of Medicare services.
| Question | Answer |
|---|---|
| Form Name | Form Insurance Agreement |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form benefits agreement, form health agreement, agreement form insurance, form insurance agreement |
DEPARTMENT OF HEALTH AND HUMAN SERVICES |
FORM APPROVED |
CENTERS FOR MEDICARE & MEDICAID SERVICES |
OMB NO. |
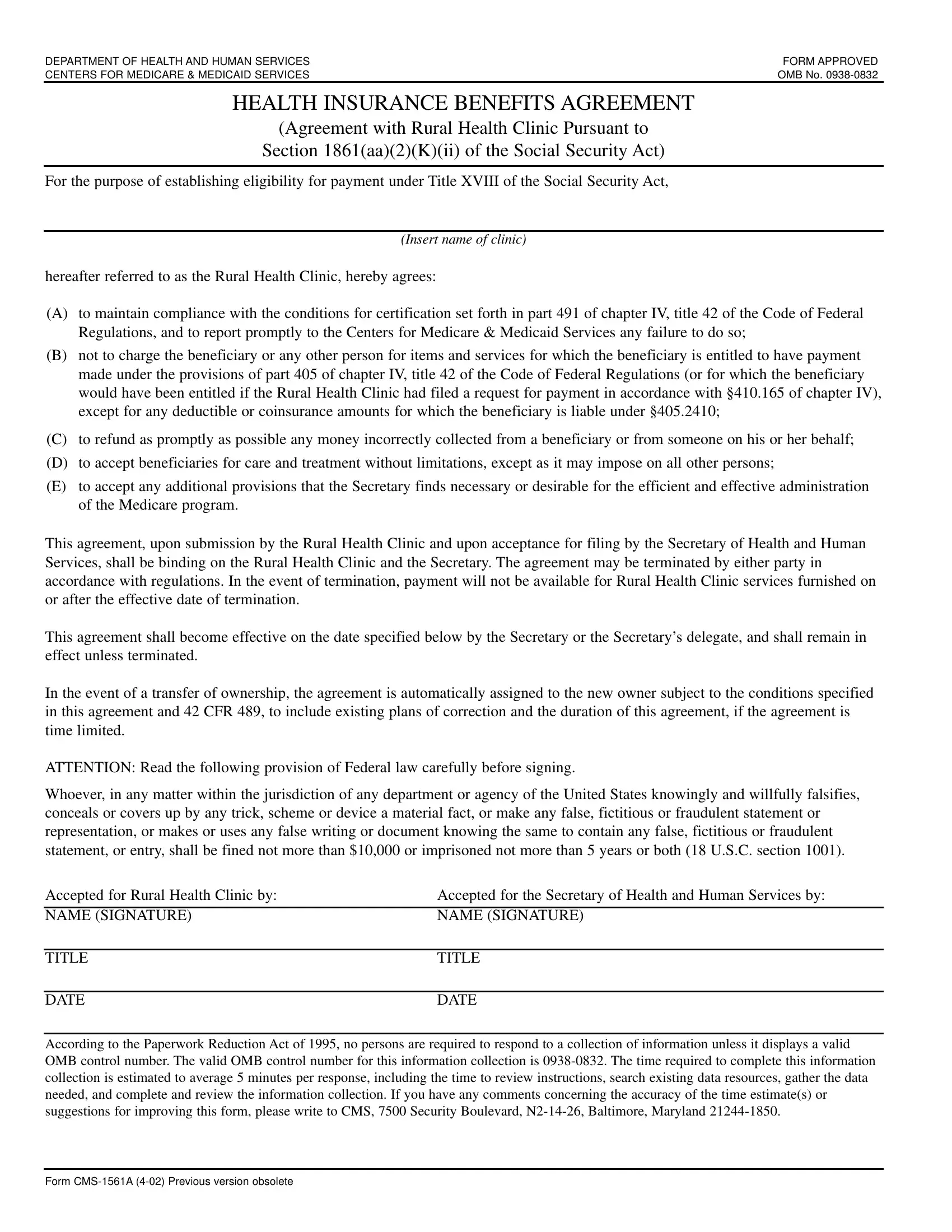
HEALTH INSURANCE BENEFITS AGREEMENT
(Agreement with Rural Health Clinic Pursuant to
Section 1861(aa)(2)(K)(ii) of the Social Security Act)
For the purpose of establishing eligibility for payment under Title XVIII of the Social Security Act,
(INSERT NAME OF CLINIC)
hereafter referred to as the Rural Health Clinic, hereby agrees:
(A)to maintain compliance with the conditions for certification set forth in part 491 of chapter IV, title 42 of the Code of Federal Regulations, and to report promptly to the Centers for Medicare & Medicaid Services any failure to do so;
(B)not to charge the beneficiary or any other person for items and services for which the beneficiary is entitled to have payment made under the provisions of part 405 of chapter IV, title 42 of the Code of Federal Regulations (or for which the beneficiary would have been entitled if the Rural Health Clinic had filed a request for payment in accordance with §410.165 of chapter IV), except for any deductible or coinsurance amounts for which the beneficiary is liable under §405.2410;
(C)to refund as promptly as possible any money incorrectly collected from a beneficiary or from someone on his or her behalf;
(D)to accept beneficiaries for care and treatment without limitations, except as it may impose on all other persons;
(E)to accept any additional provisions that the Secretary finds necessary or desirable for the efficient and effective administration of the Medicare program.
This agreement, upon submission by the Rural Health Clinic and upon acceptance for filing by the Secretary of Health and Human Services, shall be binding on the Rural Health Clinic and the Secretary. The agreement may be terminated by either party in accordance with regulations. In the event of termination, payment will not be available for Rural Health Clinic services furnished on or after the effective date of termination.
This agreement shall become effective on the date specified below by the Secretary or the Secretary’s delegate, and shall remain in effect unless terminated.
In the event of a transfer of ownership, the agreement is automatically assigned to the new owner subject to the conditions specified in this agreement and 42 CFR 489, to include existing plans of correction and the duration of this agreement, if the agreement is time limited.
ATTENTION: Read the following provision of Federal law carefully before signing.
Whoever, in any matter within the jurisdiction of any department or agency of the United States knowingly and willfully falsifies, conceals or covers up by any trick, scheme or device a material fact, or make any false, fictitious or fraudulent statement or representation, or makes or uses any false writing or document knowing the same to contain any false, fictitious or fraudulent statement, or entry, shall be fined not more than $10,000 or imprisoned not more than 5 years or both (18 U.S.C. section 1001).
Accepted for Rural Health Clinic by: |
Accepted for the Secretary of Health and Human Services by: |
|
|
NAME (SIGNATURE) |
NAME (SIGNATURE) |
|
|
TITLE |
TITLE |
|
|
DATE |
DATE |
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
FORM