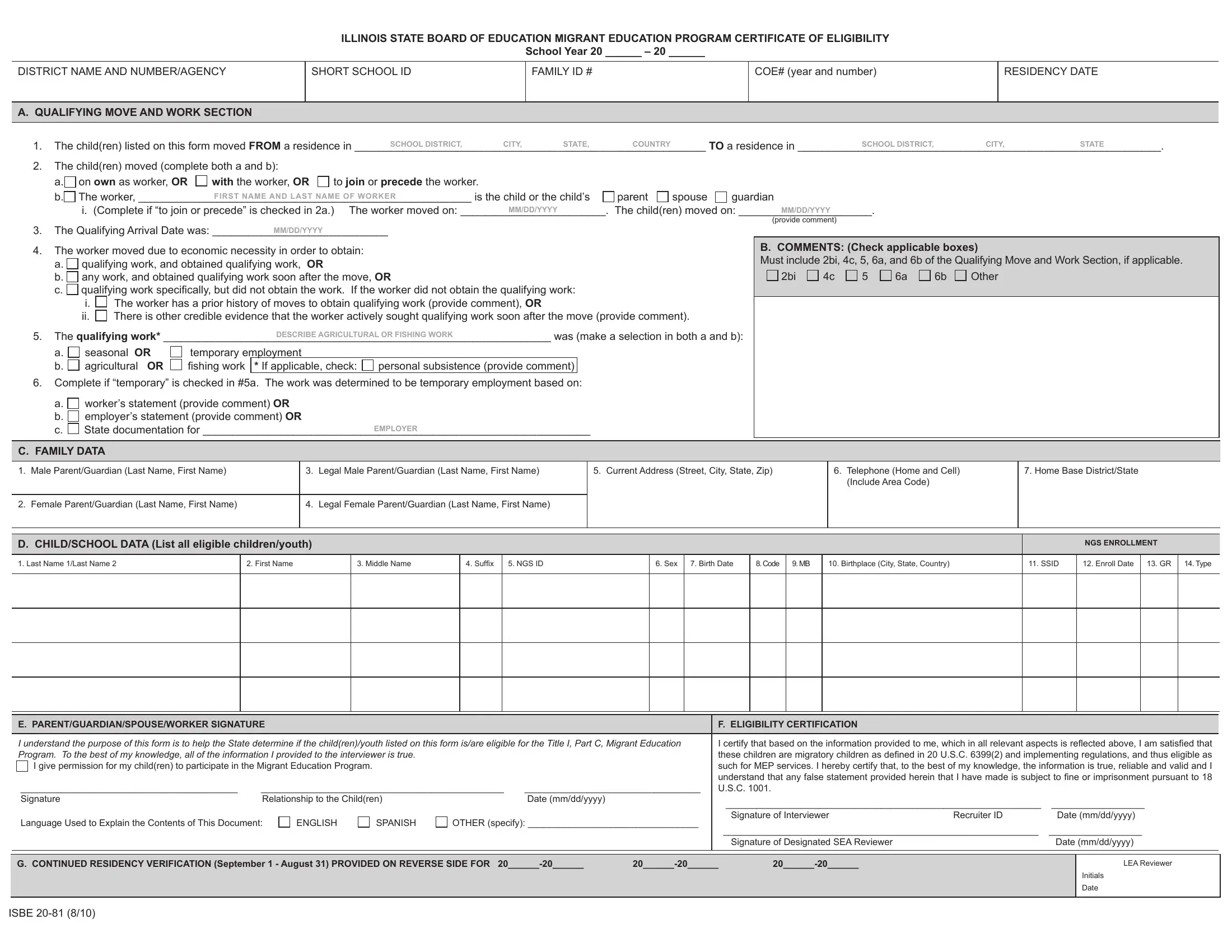
The Illinois State Board of Education's Migrant Education Program Certificate of Eligibility, commonly recognized as the ISBE 20-81 form, plays a crucial role in supporting migrant families' access to educational resources. Designed to document the eligibility of children and youth for the Title I, Part C, Migrant Education Program (MEP), this form captures detailed information about a child's migratory status, family data, educational background, and work details related to the family's moves for agricultural or fishing work. It facilitates the process by which migrant students are identified, ensuring that the necessary educational and support services can be provided. The form requires comprehensive data, including the specifics of any qualifying moves, details about the employment that necessitated the move, and personal information about the child and their guardian. Additionally, it encompasses consent sections for the continued residency verification and the release of educational and health records, safeguarding the rights and privacy of the migrant families while enabling the seamless provision of vital educational services. Through the meticulously organized sections on family data, child/school data, and eligibility certification, the ISBE 20-81 form acts as a cornerstone for ensuring that migrant children receive the educational opportunities and support they are entitled to under federal law.
| Question | Answer |
|---|---|
| Form Name | Form Isbe 20 81 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 20 81_migrant_coe school migrant certificate of eligibility online form |
ILLINOIS STATE BOARD OF EDUCATION MIGRANT EDUCATION PROGRAM CERTIFICATE OF ELIGIBILITY
School Year 20 ______ – 20 ______
DISTRICT NAME AND NUMBER/AGENCY
SHORT SCHOOL ID
FAMILY ID #
COE# (year and number)
RESIDENCY DATE
A. QUALIFYING MOVE AND WORK SECTION
1. |
The child(ren) listed on this form moved FROM a residence in |
SCHOOL DISTRICT, |
CITY, |
STATE, |
COUNTRY |
|
TO a residence in |
SCHOOL DISTRICT, |
CITY, |
STATE |
. |
|||
2. |
The child(ren) moved (complete both a and b): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. on own as worker, OR |
with the worker, OR |
to join or precede the worker. |
|
|
|
|
|
|
|
|
|
||
|
b. The worker, |
FIRST NAME AND LAST NAME OF WORKER |
is the child or the child’s |
parent |
spouse |
guardian |
|
|
|
|
||||
|
i. (Complete if “to join or precede” is checked in 2a.) The worker moved on: |
MM/DD/YYYY |
|
. The child(ren) moved on: |
MM/DD/YYYY |
. |
|
|
|
|||||
3. |
The Qualifying Arrival Date was: |
|
|
|
|
|
|
|
|
(provide comment) |
|
|
|
|
MM/DD/YYYY |
|
|
|
|
|
|
|
|
|
|
|
|
||
4.The worker moved due to economic necessity in order to obtain:
a. qualifying work, and obtained qualifying work, OR
b. any work, and obtained qualifying work soon after the move, OR
c. qualifying work speciically, but did not obtain the work. If the worker did not obtain the qualifying work:
i. The worker has a prior history of moves to obtain qualifying work (provide comment), OR
ii. There is other credible evidence that the worker actively sought qualifying work soon after the move (provide comment).
5. The qualifying work* |
|
DESCRIBE AGRICULTURAL OR FISHING WORK |
was (make a selection in both a and b): |
|||
a. |
seasonal OR |
temporary employment |
|
|
|
|
b. |
agricultural OR |
ishing work |
* If applicable, check: |
personal subsistence (provide comment) |
|
|
6.Complete if “temporary” is checked in #5a. The work was determined to be temporary employment based on:
a. worker’s statement (provide comment) OR
b. employer’s statement (provide comment) OR
c. |
State documentation for |
EMPLOYER |
B. COMMENTS: (Check applicable boxes)
Must include 2bi, 4c, 5, 6a, and 6b of the Qualifying Move and Work Section, if applicable.
2bi 4c 5 6a 6b Other
C. FAMILY DATA
1. |
Male Parent/Guardian (Last Name, First Name) |
3. |
Legal Male Parent/Guardian (Last Name, First Name) |
5. Current Address (Street, City, State, Zip) |
6. Telephone (Home and Cell) |
7. Home Base District/State |
|
|
|
|
|
(Include Area Code) |
|
|
|
|
|
|
|
|
2. |
Female Parent/Guardian (Last Name, First Name) |
4. |
Legal Female Parent/Guardian (Last Name, First Name) |
|
|
|
|
|
|
|
|
|
|
D. CHILD/SCHOOL DATA (List all eligible children/youth) |
|
|
|
|
|
|
|
|
|
NGS ENROLLMENT |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. Last Name 1/Last Name 2 |
2. First Name |
3. Middle Name |
4. Sufix |
5. NGS ID |
6. Sex |
7. Birth Date |
8. Code |
9. MB |
10. Birthplace (City, State, Country) |
11. SSID |
12. Enroll Date |
13. |
GR |
14. Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E. PARENT/GUARDIAN/SPOUSE/WORKER SIGNATURE |
|
|
|
|
F. ELIGIBILITY CERTIFICATION |
|
|
||
|
|
||||||||
I understand the purpose of this form is to help the State determine if the child(ren)/youth listed on this form is/are eligible for the Title I, Part C, Migrant Education |
I certify that based on the information provided to me, which in all relevant aspects is relected above, I am satisied that |
||||||||
Program. To the best of my knowledge, all of the information I provided to the interviewer is true. |
|
|
these children are migratory children as deined in 20 U.S.C. 6399(2) and implementing regulations, and thus eligible as |
||||||
I give permission for my child(ren) to participate in the Migrant Education Program. |
|
|
|
such for MEP services. I hereby certify that, to the best of my knowledge, the information is true, reliable and valid and I |
|||||
__________________________________________ |
_______________________________________________ |
__________________________________ |
understand that any false statement provided herein that I have made is subject to ine or imprisonment pursuant to 18 |
||||||
U.S.C. 1001. |
|
|
|||||||
Signature |
Relationship to the Child(ren) |
|
Date (mm/dd/yyyy) |
_____________________________________________________________ |
__________________ |
||||
|
|
|
|
|
|
||||
Language Used to Explain the Contents of This Document: |
ENGLISH |
SPANISH |
OTHER (specify): _________________________________ |
Signature of Interviewer |
Recruiter ID |
Date (mm/dd/yyyy) |
|||
_____________________________________________________________ |
__________________ |
||||||||
|
|
|
|
|
|
||||
|
|
|
|
|
|
Signature of Designated SEA Reviewer |
|
Date (mm/dd/yyyy) |
|
G. CONTINUED RESIDENCY VERIFICATION (September 1 - August 31) PROVIDED ON REVERSE SIDE FOR |
||
|
|
|
LEA Reviewer
Initials
Date
ISBE
|
ILLINOIS STATE BOARD OF EDUCATION MIGRANT EDUCATION PROGRAM CERTIFICATE OF ELIGIBILITY |
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
School Year 20 ______ – 20 ______ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
DISTRICT NAME AND NUMBER/AGENCY |
|
|
|
|
|
|
|
|
|
|
|
COE# (year and number) |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G. CHILD’S ETHNICITY/RACE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RACE |
|
|
|
|
|
|
|
||
|
|
|
|
ETHNICITY |
|
|
|
|
(Check one or more, regardless of ethnicity status selected.) |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
CHILD’S NAME (First and Last) |
|
|
1- Hispanic/Latino |
|
|
|
|
3- Black or |
4- Native |
|
|
|
|
|||||||||||
|
|
|
|
(Y/N) |
|
|
2- Asian |
Hawaiian or |
||||||||||||||||
|
|
|
|
|
|
|
|
Alaska Native |
|
African American |
Other Paciic |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Islander |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H. CONTINUED RESIDENCY VERIFICATION (September 1 - August 31)
School Year |
Residency Veriication |
Person Interviewed |
Relationship |
Source of Veriication |
Signature of Person Verifying |
Date |
|
Date |
(mm/dd/yyyy) |
|
|||||
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I. RELEASE OF RECORDS
The rules for migrant eligibility, services, student record transfer, and the Family Educational Rights and Privacy Act (FERPA) have been explained to me. I hereby authorize this school district, the Illinois State Board of Education (ISBE), and the New Generation System (NGS) to release, redisclose, transfer, and/or receive my child’s educational and health records, including immunization records and standardized test results, to/from other schools, educational agencies and other pertinent agencies. I know that my child’s records will be available for me to see and obtain if I so desire. In order to potentially qualify for more education, health or social services, I further consent that student/family information, otherwise conidential under the provisions of FERPA, may be shared or redisclosed to organizations that provide services under the aegis of the following: projects of the ISBE Migrant Education program (MEP), Illinois Migrant Council (IMC), College Assistance Migrant Program (CAMP), High School Equivalency Program (HEP), Migrant Education Even Start Program (MEES), Migrant Seasonal Head Start (MSHS), and child nutrition programs.
____________________________________________________________________ |
_______________________________________________ |
__________________________________ |
Signature |
Relationship to the Child(ren) |
Date (mm/dd/yyyy) |
ISBE