
Form Isbe 69 23 can be filled out without any problem. Just open FormsPal PDF editing tool to finish the job without delay. To make our tool better and more convenient to utilize, we constantly work on new features, with our users' suggestions in mind. If you are seeking to start, here is what you will need to do:
Step 1: Press the "Get Form" button at the top of this webpage to open our editor.
Step 2: Once you open the editor, you will notice the form ready to be filled in. In addition to filling in different blank fields, you could also perform several other things with the file, particularly writing any textual content, modifying the original textual content, inserting illustrations or photos, signing the PDF, and more.
With regards to the fields of this particular PDF, this is what you need to know:
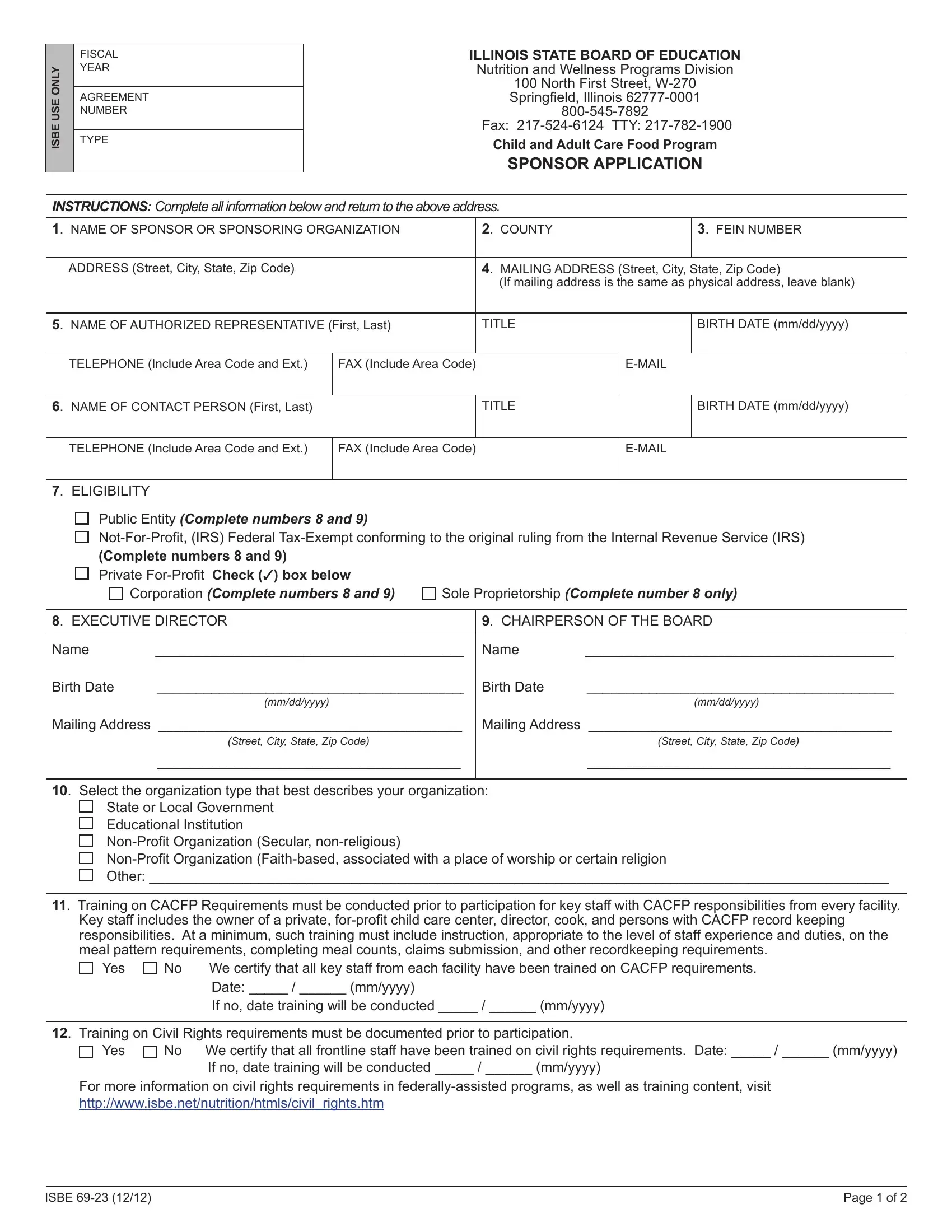
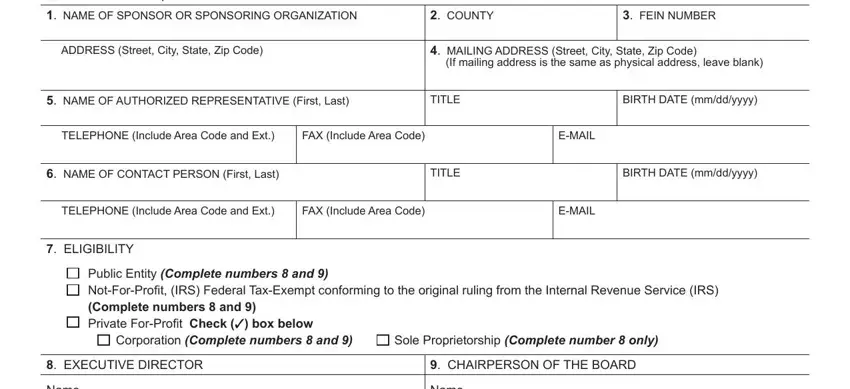
1. It is recommended to fill out the Form Isbe 69 23 accurately, therefore take care when filling in the parts including all of these fields:
2. The subsequent part is usually to fill in these particular blanks: Name, Name, Birth Date mmddyyyy, Birth Date mmddyyyy, Mailing Address Street City State, Mailing Address Street City State, Select the organization type that, Training on CACFP Requirements, and Training on Civil Rights.
Concerning Training on Civil Rights and Select the organization type that, make sure that you get them right in this section. Those two are definitely the key fields in this file.
3. In this specific stage, have a look at CommoditySponsor Elects The box, MultiState organizations Does, Audit Information During this, DUNS Number Dun and, Yes No Will your organization, and Yes No Do you agree to send this. Each one of these have to be filled out with highest attention to detail.
4. Filling in Yes No Do you agree to send this, Yes No Do you agree to submit a, Other, I certify that neither the, and Date Original Signature of is key in this next step - make certain that you don't hurry and fill out every single field!
Step 3: Immediately after going through your entries, hit "Done" and you're done and dusted! Create a 7-day free trial plan with us and get instant access to Form Isbe 69 23 - accessible from your personal account page. FormsPal provides risk-free document tools without personal data record-keeping or sharing. Rest assured that your details are safe with us!