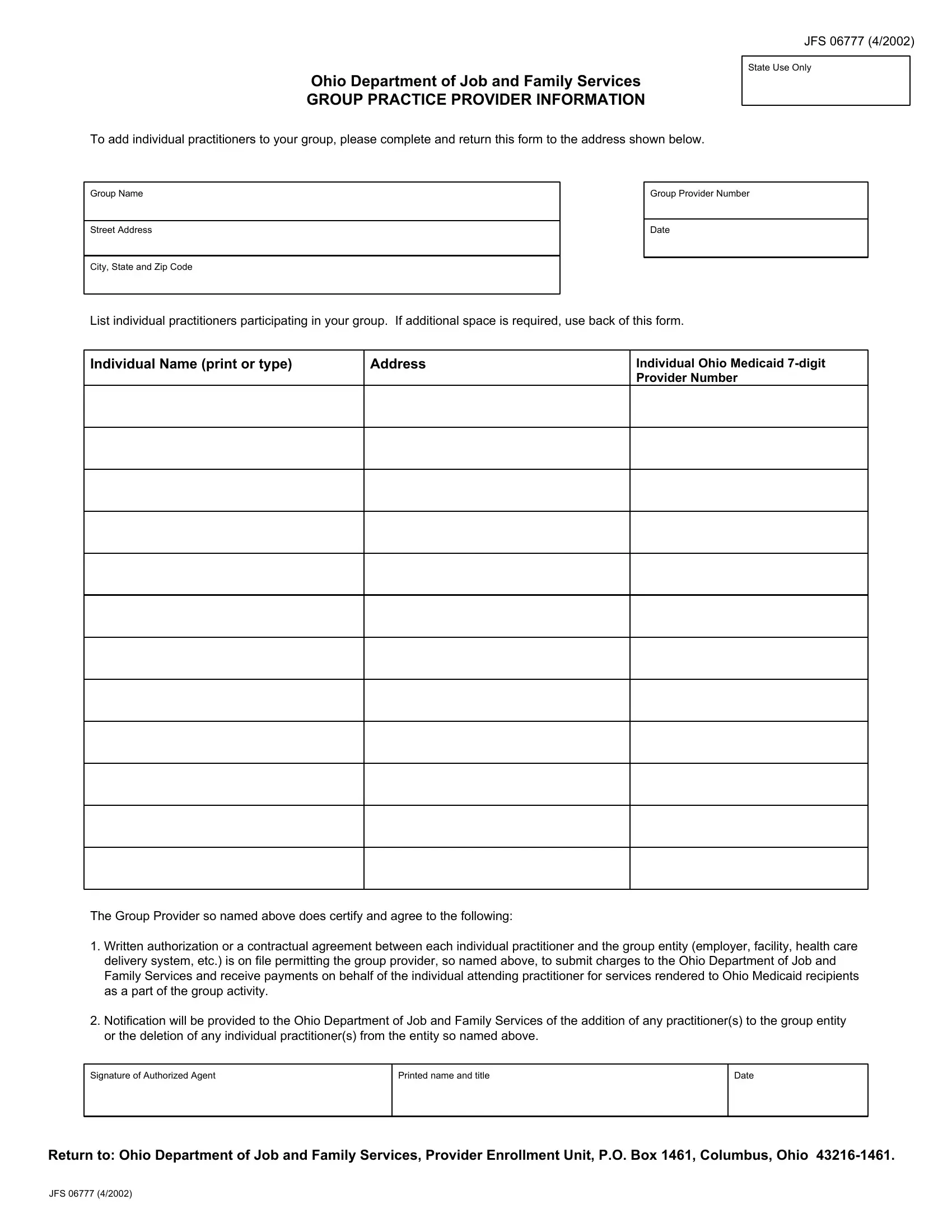
In the landscape of healthcare provision and management, particularly within Ohio, the JFS 06777 form stands as a pivotal document for group practices aiming to streamline the addition of individual practitioners. Issued by the Ohio Department of Job and Family Services, this form serves as a conduit for group practices to officially include new practitioners in their roster, ensuring that the administrative facets of healthcare delivery are in lockstep with regulatory requirements. The essence of the form revolves around providing detailed information about each practitioner being added, including their name, address, and individual Ohio Medicaid 7-digit Provider Number. It mandates a declaration from the group provider, acknowledging that a written authorization or contractual agreement is in place for every practitioner listed, thereby enabling the group entity to forward charges to, and receive payments from, the Ohio Department of Job and Family Services for services rendered to Ohio Medicaid recipients. Furthermore, the form embodies a commitment by the group provider to notify the Ohio Department of Job and Family Services regarding any changes in the group's composition, such as additions or deletions of practitioners. The process culminates in the submission of the form to the Provider Enrollment Unit, marking a crucial step in managing healthcare provision within a regulatory framework that emphasizes accountability and orderly administration.
| Question | Answer |
|---|---|
| Form Name | Form Jfs 06777 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | groupinfo ohio job family services form |
Ohio Department of Job and Family Services
GROUP PRACTICE PROVIDER INFORMATION
To add individual practitioners to your group, please complete and return this form to the address shown below.
JFS 06777 (4/2002)
State Use Only
Group Name
Street Address
City, State and Zip Code
Group Provider Number
Date
List individual practitioners participating in your group. If additional space is required, use back of this form.
Individual Name (print or type)
Address
Individual Ohio Medicaid
The Group Provider so named above does certify and agree to the following:
1.Written authorization or a contractual agreement between each individual practitioner and the group entity (employer, facility, health care delivery system, etc.) is on file permitting the group provider, so named above, to submit charges to the Ohio Department of Job and Family Services and receive payments on behalf of the individual attending practitioner for services rendered to Ohio Medicaid recipients as a part of the group activity.
2.Notification will be provided to the Ohio Department of Job and Family Services of the addition of any practitioner(s) to the group entity or the deletion of any individual practitioner(s) from the entity so named above.
Signature of Authorized Agent
Printed name and title
Date
Return to: Ohio Department of Job and Family Services, Provider Enrollment Unit, P.O. Box 1461, Columbus, Ohio
JFS 06777 (4/2002)