Form L 1 1 is an important form that every business owner should be familiar with. This form is used to report income and expenses to the Internal Revenue Service (IRS). By understanding how to complete this form, you can ensure that you are reporting all of your income and expenses accurately. In this blog post, we will walk you through how to fill out Form L 1 1 correctly. We will also provide some tips for ensuring accuracy and completeness. Let's get started!
| Question | Answer |
|---|---|
| Form Name | Form L 1 1 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | NewJersey state of new jersey employers first report of accidental injury or occupational illness form |
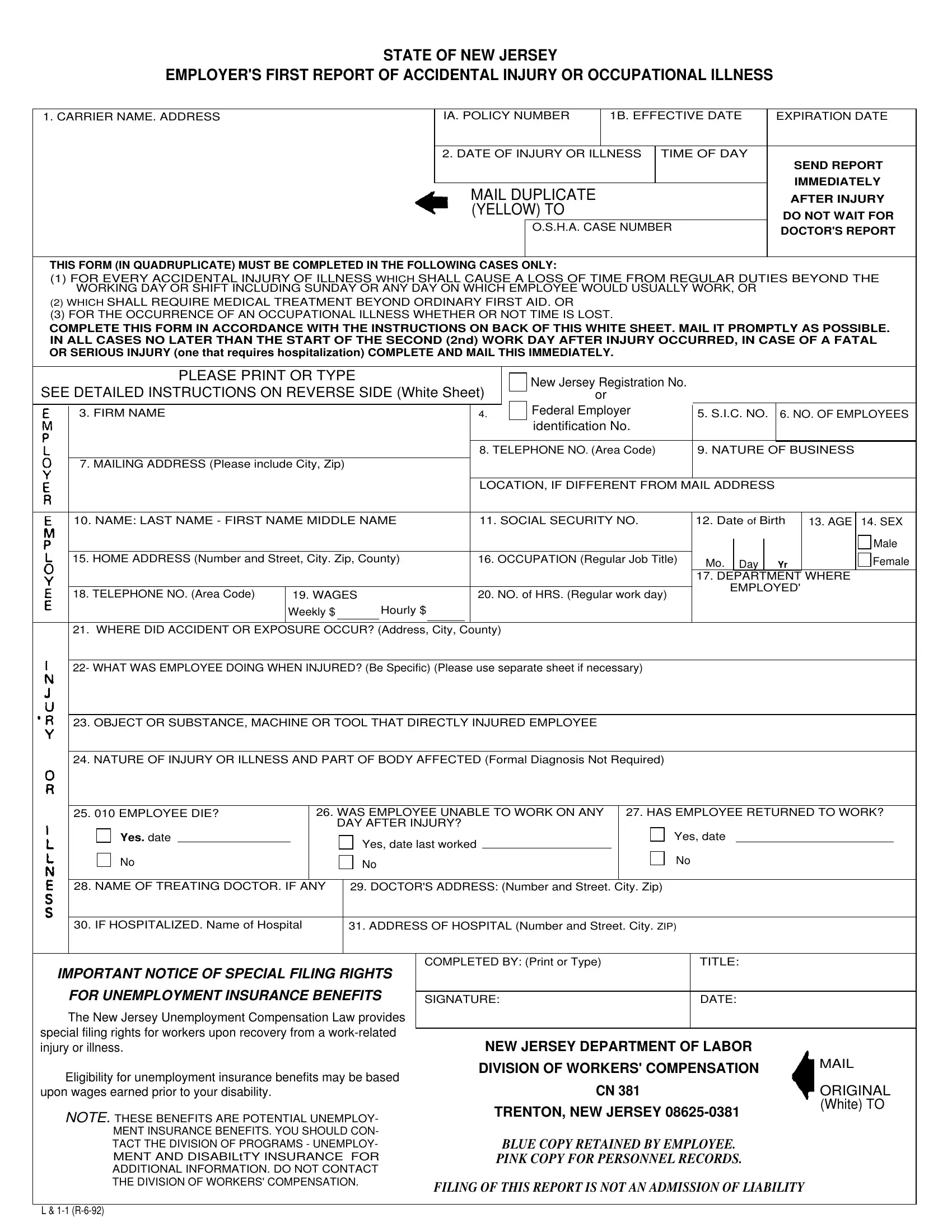
STATE OF NEW JERSEY
EMPLOYER'S FIRST REPORT OF ACCIDENTAL INJURY OR OCCUPATIONAL ILLNESS
1. CARRIER NAME. ADDRESS
IA. POLICY NUMBER |
1B. EFFECTIVE DATE |
EXPIRATION DATE |
||
|
|
|
|
|
2. DATE OF INJURY OR ILLNESS |
TIME OF DAY |
|
||
|
|
|
|
SEND REPORT |
|
|
|
|
IMMEDIATELY |
MAIL DUPLICATE |
|
|
||
|
|
AFTER INJURY |
||
(YELLOW) TO |
|
|
DO NOT WAIT FOR |
|
|
O.S.H.A. CASE NUMBER |
DOCTOR'S REPORT |
||
|
|
|
|
|
|
|
|
|
|
THIS FORM (IN QUADRUPLICATE) MUST BE COMPLETED IN THE FOLLOWING CASES ONLY:
(1)FOR EVERY ACCIDENTAL INJURY OF ILLNESS WHICH SHALL CAUSE A LOSS OF TIME FROM REGULAR DUTIES BEYOND THE WORKING DAY OR SHIFT INCLUDING SUNDAY OR ANY DAY ON WHICH EMPLOYEE WOULD USUALLY WORK, OR
(2)WHICH SHALL REQUIRE MEDICAL TREATMENT BEYOND ORDINARY FIRST AID. OR
(3)FOR THE OCCURRENCE OF AN OCCUPATIONAL ILLNESS WHETHER OR NOT TIME IS LOST.
COMPLETE THIS FORM IN ACCORDANCE WITH THE INSTRUCTIONS ON BACK OF THIS WHITE SHEET. MAIL IT PROMPTLY AS POSSIBLE. IN ALL CASES NO LATER THAN THE START OF THE SECOND (2nd) WORK DAY AFTER INJURY OCCURRED, IN CASE OF A FATAL OR SERIOUS INJURY (one that requires hospitalization) COMPLETE AND MAIL THIS IMMEDIATELY.
|
PLEASE PRINT OR TYPE |
|
|
|
|
New Jersey Registration No. |
|
|
|
|
|
|
||
SEE DETAILED INSTRUCTIONS ON REVERSE SIDE (White Sheet) |
|
|
|
|
|
|
||||||||
or |
|
|
|
|
|
|
||||||||
|
3. FIRM NAME |
|
|
|
|
|
4. |
Federal Employer |
5. S.I.C. NO. |
6. NO. OF EMPLOYEES |
||||
|
|
|
|
|
|
|
|
identification No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. TELEPHONE NO. (Area Code) |
9. NATURE OF BUSINESS |
|
|||||
|
7. MAILING ADDRESS (Please include City, Zip) |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LOCATION, IF DIFFERENT FROM MAIL ADDRESS |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
10. NAME: LAST NAME - FIRST NAME MIDDLE NAME |
11. SOCIAL SECURITY NO. |
12. Date of Birth |
13. AGE |
14. SEX |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. HOME ADDRESS (Number and Street, City. Zip, County) |
16. OCCUPATION (Regular Job Title) |
Mo. |
Day |
|
Yr |
|
Female |
||||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
17. DEPARTMENT WHERE |
|
||||
|
|
|
|
|
|
|
|
|
EMPLOYED' |
|
||||
|
18. TELEPHONE NO. (Area Code) |
19. WAGES |
|
|
|
20. NO. of HRS. (Regular work day) |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Weekly $ |
Hourly $ |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. WHERE DID ACCIDENT OR EXPOSURE OCCUR? (Address, City, County) |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
22- WHAT WAS EMPLOYEE DOING WHEN INJURED? (Be Specific) (Please use separate sheet if necessary) |
|
|
|
|
|
|
|||||||
23.OBJECT OR SUBSTANCE, MACHINE OR TOOL THAT DIRECTLY INJURED EMPLOYEE
24.NATURE OF INJURY OR ILLNESS AND PART OF BODY AFFECTED (Formal Diagnosis Not Required)
|
25. 010 EMPLOYEE DIE? |
26. WAS EMPLOYEE UNABLE TO WORK ON ANY |
27. HAS EMPLOYEE RETURNED TO WORK? |
||||||||||||
|
|
|
|
|
DAY AFTER INJURY? |
|
|
|
|
|
|
||||
|
Yes. date |
|
|
|
|
Yes, date last worked |
|
Yes, date |
|
|
|
||||
|
No |
|
|
|
No |
|
|
||||||||
|
|
|
No |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
28. NAME OF TREATING DOCTOR. IF ANY |
|
29. DOCTOR'S ADDRESS: (Number and Street. City. Zip) |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
30. IF HOSPITALIZED. Name of Hospital |
|
|
31. ADDRESS OF HOSPITAL (Number and Street. City. ZIP) |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLETED BY: (Print or Type) |
|
TITLE: |
|
|
||||
IMPORTANT NOTICE OF SPECIAL FILING RIGHTS |
|
|
|
|
|
|
|
|
|
||||||
|
FOR UNEMPLOYMENT INSURANCE BENEFITS |
|
|
|
|
|
|
|
|
|
|||||
|
SIGNATURE: |
|
DATE: |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||||
The New Jersey Unemployment Compensation Law provides |
|
|
|
|
|
|
|
|
|
||||||
special filing rights for workers upon recovery from a |
|
|
|
|
|
|
|
|
|
||||||
|
NEW JERSEY DEPARTMENT OF LABOR |
|
|
||||||||||||
injury or illness. |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
DIVISION OF WORKERS' COMPENSATION |
||||||||
Eligibility for unemployment insurance benefits may be based |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|||||||
upon wages earned prior to your disability. |
|
|
|
|
CN 381 |
|
|
|
ORIGINAL |
||||||
|
|
|
|
|
|
|
|
TRENTON, NEW JERSEY |
(White) TO |
||||||
NOTE. THESE BENEFITS ARE POTENTIAL UNEMPLOY- |
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|||||||
|
MENT INSURANCE BENEFITS. YOU SHOULD CON- |
|
|
|
|
|
|
|
|
|
|||||
|
TACT THE DIVISION OF PROGRAMS - UNEMPLOY- |
|
BLUE COPY RETAINED BY EMPLOYEE. |
|
|
||||||||||
|
MENT AND DISABILtTY INSURANCE FOR |
|
PINK COPY FOR PERSONNEL RECORDS. |
|
|
||||||||||
|
ADDITIONAL INFORMATION. DO NOT CONTACT |
|
|
|
|
|
|
|
|
|
|||||
THE DIVISION OF WORKERS' COMPENSATION. |
FILING OF THIS REPORT IS NOT AN ADMISSION OF LIABILITY |
|
L &
INSTRUCTIONS
1 . CARRIER NAME, ADDRESS: Indicate the name and address of the firm's Workers' Compensation carrier. if
1A. POLICY NUMBER: Indicate the firm's Workers' Compensation Insurance policy number.
1B. EFFECTIVE DATE: Indicate the date when the present policy started. EXPIRATION DATE: Indicate the date when the present policy expires.
2.DATE OF INJURY OR ILLNESS: Indicate the date when the injury occurred or in case of illness, when first detected. TIME OF DAY: Indicate the time of injury or illness (i.e. 9:30 a.m. or 7:00 p.m.)
O.S.H.A. CASE NUMBER: (Leave Blank)
3.FIRM NAME: Indicate the full name of individual, partnership, corporation or trade name of the employer.
4.NEW JERSEY REGISTRATION NUMBER OR FEDERAL EMPLOYER IDENTIFICATION NUMBER: Indicate either your company's New Jersey Registration Number or your company's Federal Employer Identification Number. This number can be obtained from your copy of Quarterly Report of Wages (Form U.C. 27B). The account number is on the fifth line of the address.
S. S.I.C. Number: Indicate the S.I.C. Number of your firm. This number can be obtained from your copy of Quarterly Report of Wages (Form U.C. 27B). The S.I.C. isthe four digit number in the lower right hand corner of the address under the account number.
6.NO. OF EMPLOYEES: The number of employees employed by the firm.
7.MAILING ADDRESS: The address of the employer.
8.TELEPHONE NO. (AREA CODE): The business telephone of the employer.
9.NATURE OF BUSINESS: Describe the kind of business of the employer, i.e. manufacture shoes, wholesale food, retail clothing, construction, transportation, communication, utilities, government, etc.
LOCATION, IF DIFFERENT FROM MAILING ADDRESS: If the location where the injury or illness occurred is different from the mailing address of the employer in question #3.
10.NAME: Indicate the full name of the employee as carried on payroll records.
11.SOCIAL SECURITY NO.: Indicate the Social Security number of the employee.
12. DATE OF BIRTH: |
13. AGE: |
14. SEX: |
15.HOME ADDRESS: The address of the employee.
16.OCCUPATION: The job classification of employee, i.e., carpenter, electrician, driver, lathe operator, salesperson, etc.
17.
18.TELEPHONE
19.WAGES: if employee is paid weekly salary indicate gross weekly amount. If employee is paid hourly indicate hourly rate. (exclude overtime)
20.NO. OF HOURS: Indicate the total regular number of hours employee works per day. (exclude overtime)
21.WHERE DID ACCIDENT OR EXPOSURE OCCUR? If the location of accident or exposure is different from the address shown on line 7, give sufficient information to pinpoint location by giving address, city, county, route orjob location.
22.WHAT WAS EMPLOYEE DOING WHEN INJURED? Examples: walking down stairs, climbing ladder, operating table saw, changing wheel on grinder, sitting at desk, opening file drawer, etc.
23.OBJECT OR SUBSTANCE, MACHINE OR TOOL THAT DIRECTLY INJURED EMPLOYEE Examples: stairs and handrail, floor, saw blade, dust, vapors, chips, chisel, hammer, chain, acid (name), steam, fire, hot sluge, electric current, the item employee was lifting, pushing or pulling, etc.
24.NATURE OF INJURY OR ILLNESS AND PART OF BODY AFFECTED Examples: amputation of right index finger, fracture of ribs, burn of left hand, contusions of both legs, laceration of upper right arm, etc.
Examples of occupational disease: dermatitis of neck, silicosis, etc.
25.DID EMPLOYEE DIE? Was the injury or illness the cause of death?
26.WAS EMPLOYEE UNABLE TO WORK ON ANY DAY AFTER INJURY?
27.HAS EMPLOYEE RETURNED TO WORK?
28, 29, 30, 31