We've applied the efforts of our best developers to make the PDF editor you may want to take advantage of. The software will assist you to create the L-1124 form without trouble and don’t waste your time. Everything you should do is try out these particular straightforward recommendations.
Step 1: Press the "Get Form Now" button to begin.
Step 2: At the moment, you may update your L-1124. Our multifunctional toolbar enables you to add, erase, alter, highlight, and also carry out other commands to the content and areas inside the file.
All of these sections are included in the PDF document you'll be creating.
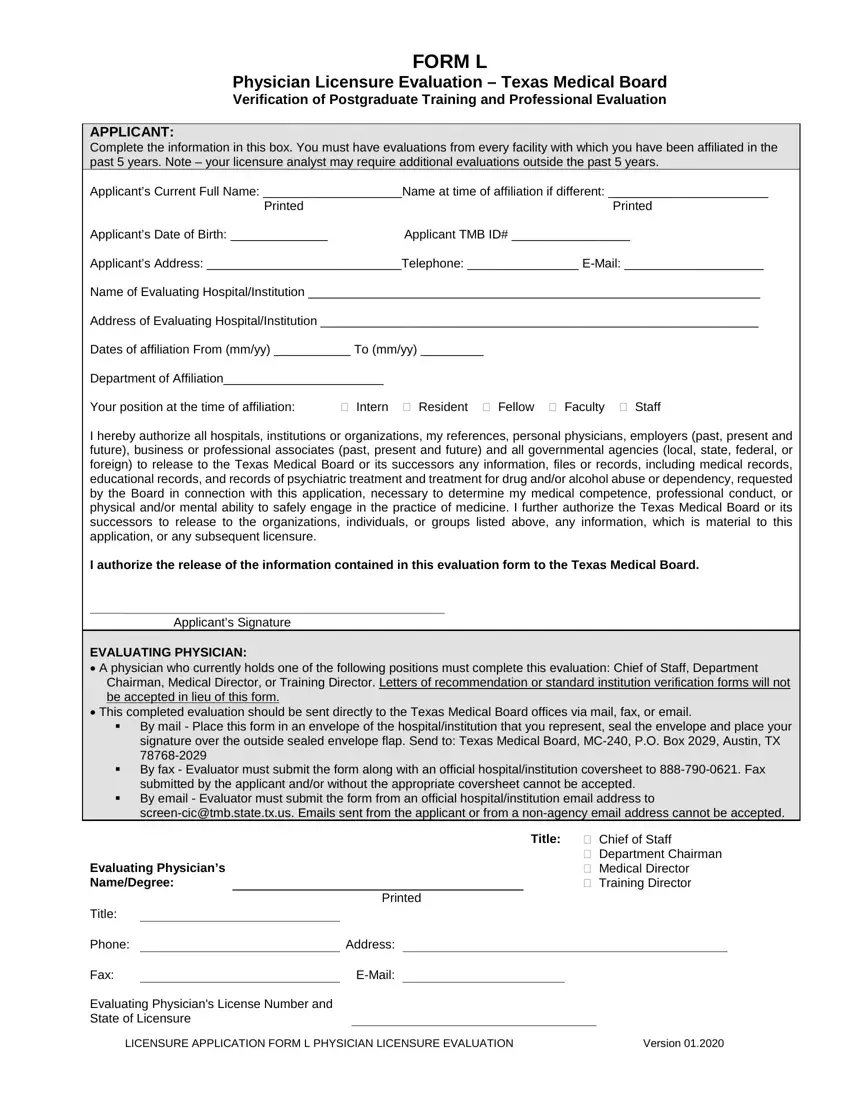
In the Title Chief of Staff, Department Chairman Medical, Evaluating Physicians NameDegree, Title, Phone, Fax, Printed, Address, EMail, Evaluating Physicians License, and LICENSURE APPLICATION FORM L box, note down your data.
Inside the field dealing with FORM L, Applicants Name Printed, Page, This is important All information, FOR TRAINING POSITIONS Completion, FOR NONTRAINING POSITIONS Only, VERIFICATION OF POST GRADUATE, PROGRAM PARTICIPATION For training, Report incomplete postgraduate, If the postgraduate year is, Report Internships Residencies and, PGY Internship Residency, PGY Internship Residency, Department, and From, it's essential to put down some appropriate data.
As part of field Report Internships Residencies and, PGY Internship Residency, From, Credit received, Full, Partial, in progress, For partial credit how many months, Department, PGY Internship Residency, From, Credit received, Full, Partial, and in progress, specify the rights and responsibilities.
Check the areas Applicants Name, Page, VERIFICATION OF PROFESSIONAL, This evaluation is based on, Review of Credential File, How long have you known the, Is the applicant related to you, Do you know the applicant well, Yes, Yes, Has your acquaintance with the, Yes, Do you consider the applicant, a Reliable b Ethical c Of good, and Please rate the applicant and then complete them.
Step 3: Choose "Done". Now you can upload your PDF form.
Step 4: You should create as many copies of the form as possible to stay away from future misunderstandings.
