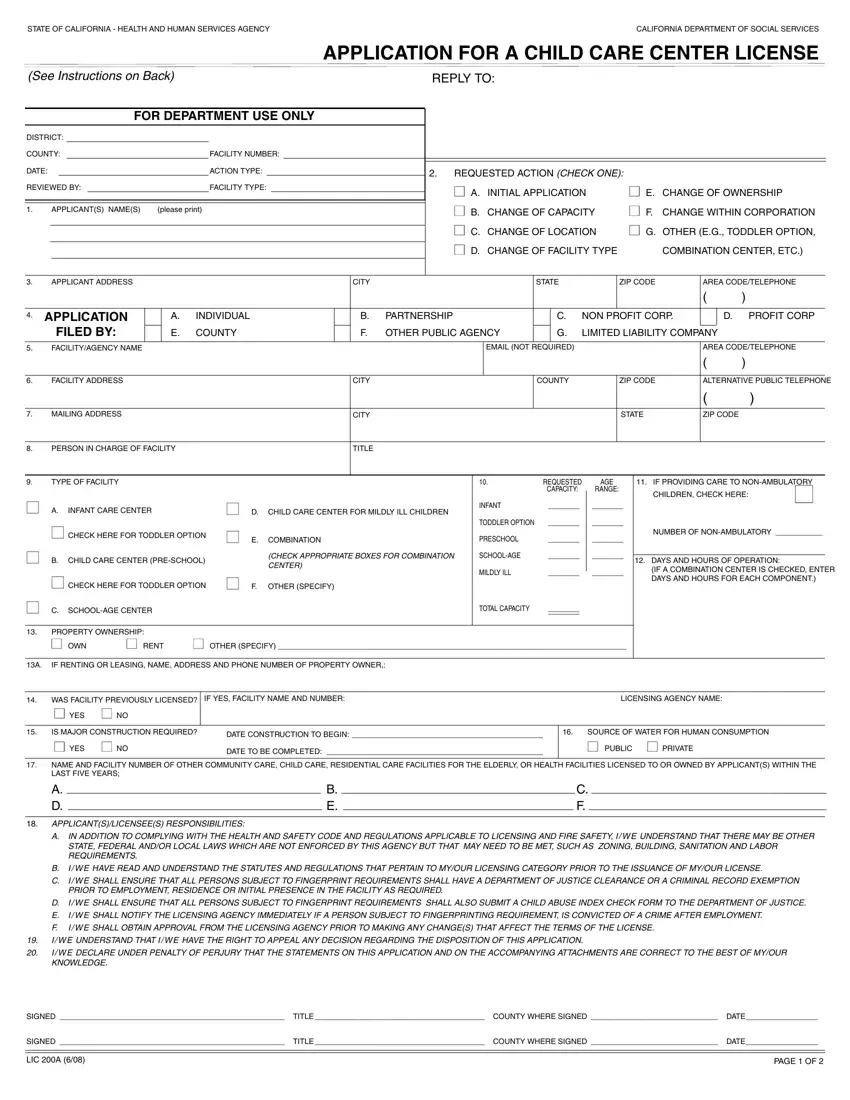
Type or print clearly. Prepare application in duplicate. Return original.
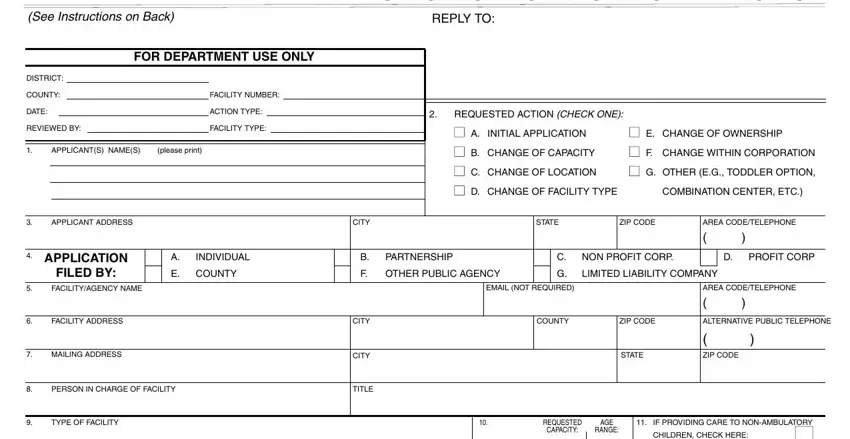
1.Applicant(s): Enter the name(s) of the person(s) or organization legally responsible for the facility. Enter full names. Individuals enter first, middle and last name. If joint application, all applicants must sign this application. Individuals, each partner, and chief executive officer or authorized representative of a firm, association, corporation, county, city, public agency or governmental entity must complete Applicant Information (LIC 215). Corporations and other organizations also complete Administrative Organization, (LIC 309).
2.Requested Action: Check appropriate box.
3.Applicant Address: Enter legal home address of individual(s) and headquarters address of corporations. Major partner enters principal business address. Other partners enter principal business address on Applicant Information (LIC 215). Enter area code with telephone number.
4.Application Filed by: Check appropriate box.
5.Facility/Agency Name: Enter the name used to designate the single facility under application. If an agency, fill in the name of the agency which provides the services and hyphenate the single facility name, e.g., YMCA-Peppertree Day Care School.
6.Facility Address: Enter the address of the physical location of the facility. If applicant has more than one facility, a separate application must be completed for each facility. Enter area code with telephone number.
7.Mailing Address: Enter the address where all mail from the department/licensing agency should be sent.
8.Person in Charge of Facility: Enter the name and title of person who will directly supervise the facility. If not yet employed, enter “Unknown.”
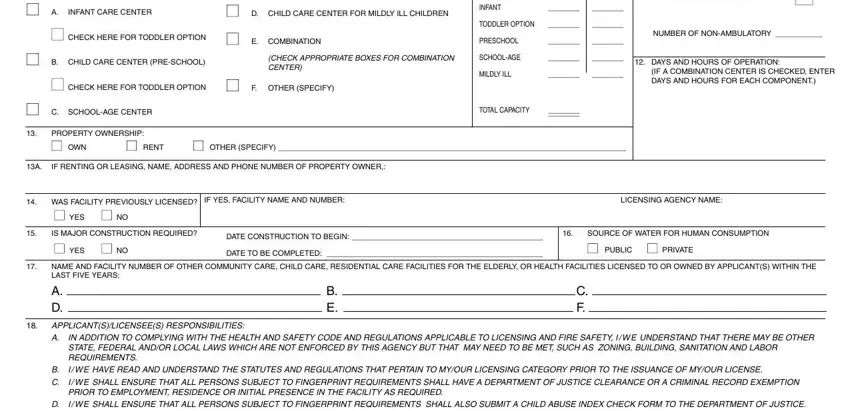
9.Type of Facility: Check the appropriate box for type of facility as defined in California Code of Regulations, Title 22.
10.Requested Capacity and Age Range: Enter the total number of children and age range for whom care will be provided at any time.
11.Check box and enter number of non-ambulatory children for which you are providing care.
12.Days & Hours of Operation: Enter days and hours of operation of facility.
13.Property Ownership: Check the appropriate box.
13A. Control of Property: If applicant(s) is leasing or renting, enter name, address and phone of owner of facility premises.
14.Was Facility Previously Licensed? Check YES or NO. If yes, enter facility name, number and name of agency which issued license(s).
15.Is Facility to be Constructed or Require Major Building Change? Self-explanatory.
16.Source of Water for Human Consumption: Check PUBLIC or PRIVATE water source.
17.Other Facilities: Enter the facility name and number of any other community care or health facilities owned or operated by applicant(s).
18.Statement of applicant(s)/licensee(s) responsibilities of compliance with all applicable laws and regulations.
19.Acknowledgement of right to appeal.
20.Signatures of all applicants or authorized person(s) (e.g., general partners of a partnership and executive officer or duly authorized representative for all corporations, public agencies, etc.).