

Through the online editor for PDFs by FormsPal, you can easily complete or modify admission agreement pdf here. Our tool is continually evolving to provide the best user experience attainable, and that is due to our resolve for constant development and listening closely to customer comments. Here's what you will have to do to begin:
Step 1: Open the PDF inside our tool by clicking on the "Get Form Button" in the top section of this webpage.
Step 2: The tool provides you with the opportunity to customize PDF files in various ways. Transform it with your own text, adjust what is originally in the file, and include a signature - all when it's needed!
If you want to finalize this PDF document, ensure that you type in the necessary information in each field:
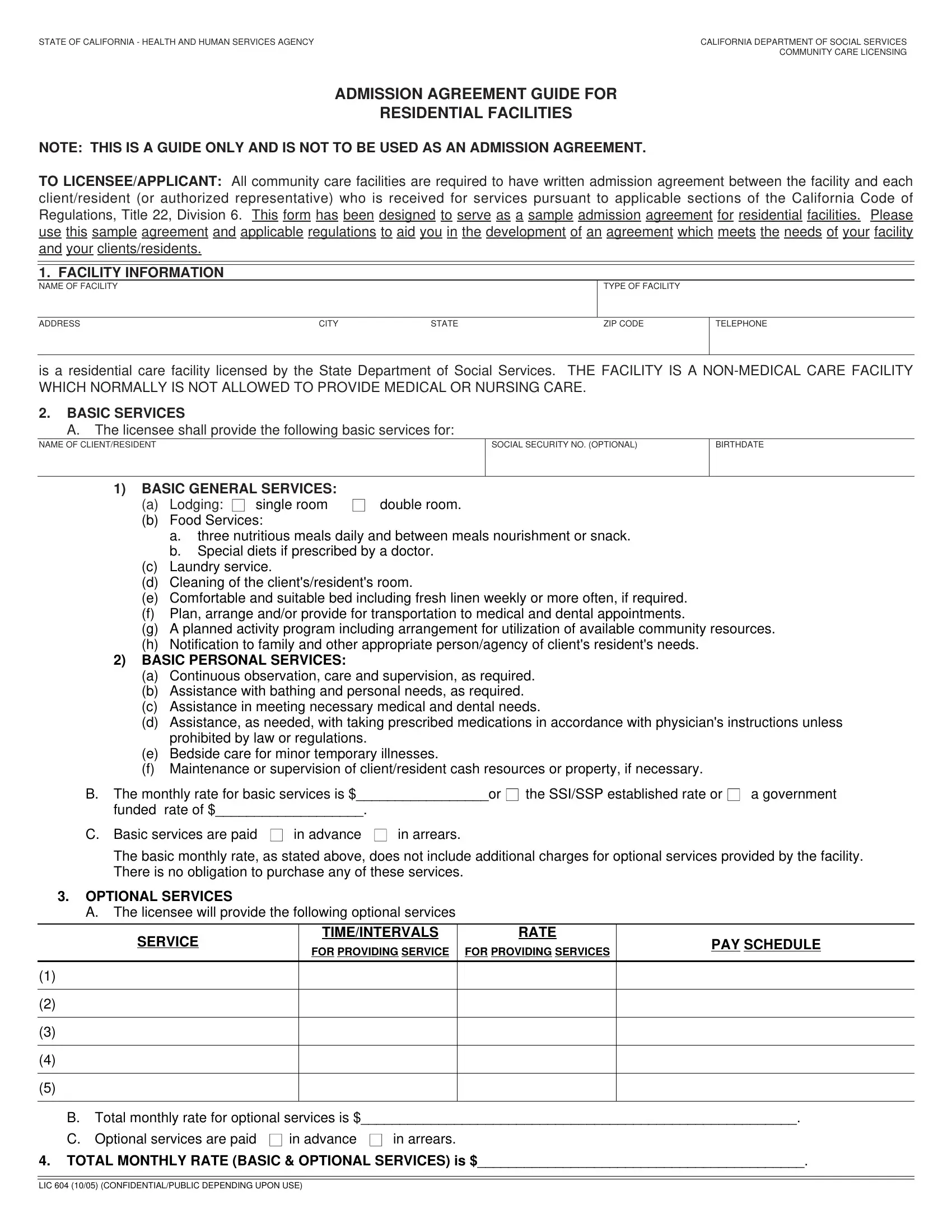
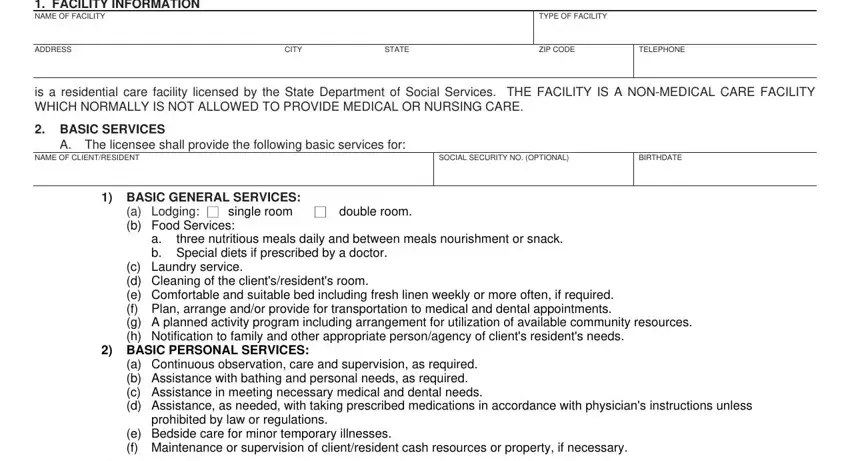
1. To start off, while filling out the admission agreement pdf, begin with the section with the subsequent fields:
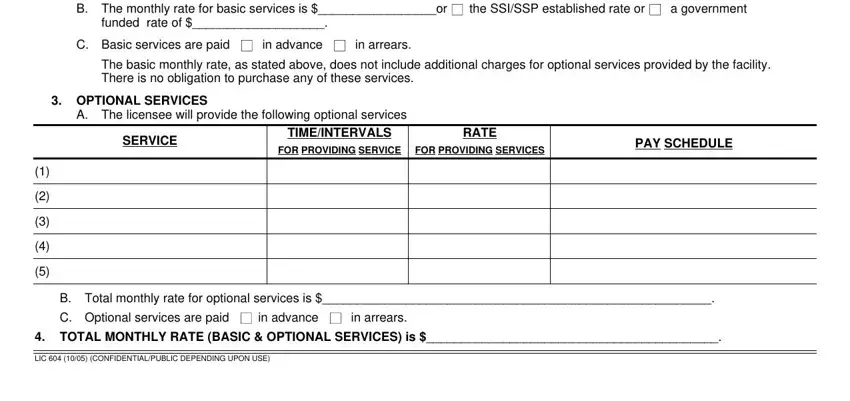
2. Just after finishing the previous step, head on to the next step and complete all required particulars in all these blank fields - B The monthly rate for basic, the SSISSP established rate or, a government, funded rate of in advance, C Basic services are paid, in arrears, The basic monthly rate as stated, OPTIONAL SERVICES, A The licensee will provide the, SERVICE, TIMEINTERVALS, RATE, FOR PROVIDING SERVICE, FOR PROVIDING SERVICES, and PAY SCHEDULE.
3. The third part will be hassle-free - fill in every one of the empty fields in or more of the following reasons, Failure of the clientresident to, Change of use of the facility, B The licenseeadministrator of the, C The licenseeadministrator of the, FACILITY VISITING POLICY The, DISCHARGEREMOVAL GROUP HOMES The, and NOTICE OF RATE CHANGE If rates to complete the current step.
4. Filling in admission to or departure from the, REFUND POLICY Refund policy for, If clientresident leave the, The licensee will not be, delivered to the, will, NAME OF CLIENTRESIDENT OR, Will, A Pay the basic monthly rate B C, will not purchase the above listed, in advance, in arrears, Provide two weeks notice of intent, California Code of Regulations, and The right of the licensing agency is vital in the fourth part - don't forget to take the time and fill out every empty field!
People who work with this form often get some things incorrect when filling in The right of the licensing agency in this section. Remember to re-examine what you enter here.
5. To finish your document, this particular segment involves a couple of extra blanks. Filling out LICENSEEADMINISTRATOR, AUTHORIZED REPRESENTATIVE, DATE, DATE, and Admission agreements and any will certainly conclude the process and you'll be done in no time at all!

Step 3: Before moving forward, double-check that all form fields are filled in properly. When you verify that it is good, click on “Done." After getting afree trial account with us, you'll be able to download admission agreement pdf or send it via email promptly. The document will also be easily accessible from your personal account page with your every modification. FormsPal ensures your data privacy by using a secure method that never saves or distributes any kind of private information used. Rest assured knowing your docs are kept safe when you work with our editor!