
TODAYS can be completed online without difficulty. Simply make use of FormsPal PDF editor to perform the job in a timely fashion. To make our editor better and simpler to utilize, we constantly develop new features, considering feedback coming from our users. All it takes is a couple of basic steps:
Step 1: Hit the "Get Form" button at the top of this webpage to access our PDF tool.
Step 2: When you launch the editor, there'll be the document made ready to be filled in. Other than filling out different blanks, you could also perform other things with the Document, particularly writing any text, changing the original textual content, adding images, affixing your signature to the form, and a lot more.
This form will involve some specific information; in order to guarantee accuracy and reliability, please take into account the recommendations below:
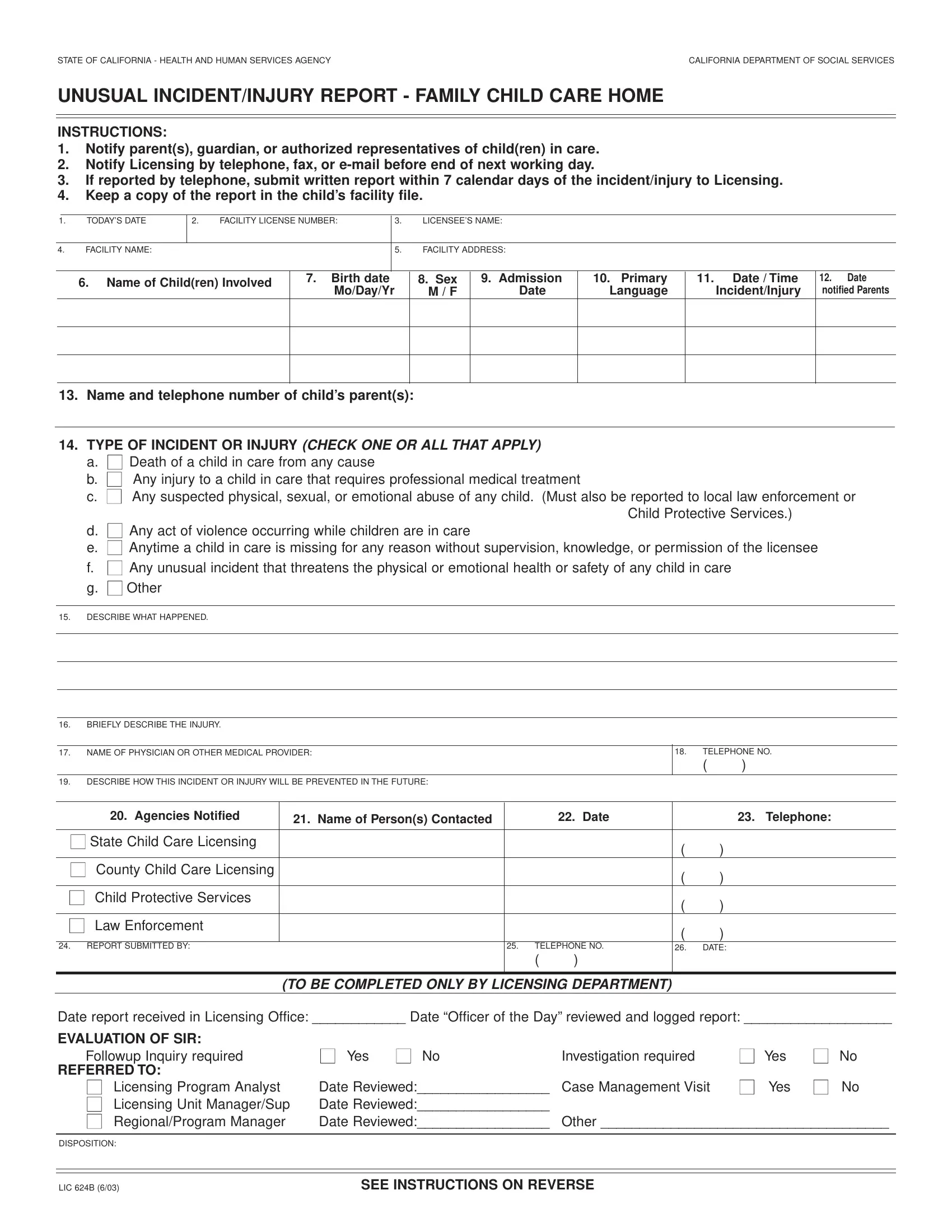
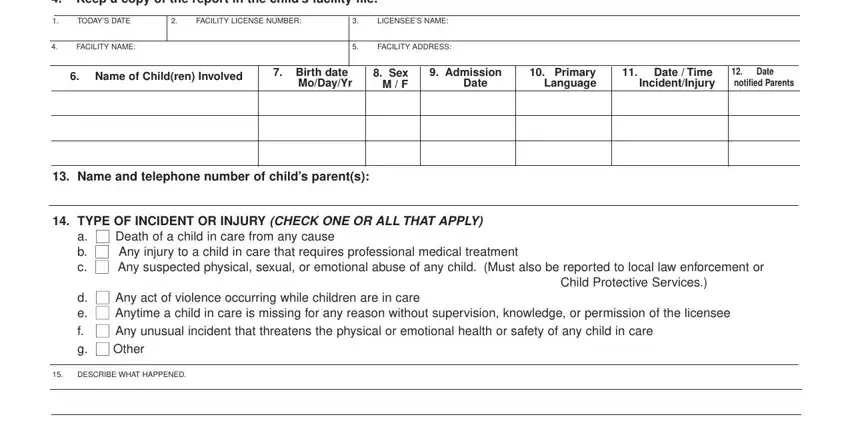
1. The TODAYS requires certain details to be entered. Be sure the following fields are filled out:
2. When this part is done, you're ready include the needed details in BRIEFLY DESCRIBE THE INJURY, NAME OF PHYSICIAN OR OTHER MEDICAL, DESCRIBE HOW THIS INCIDENT OR, TELEPHONE NO, Agencies Notified, Name of Persons Contacted, Date, Telephone, State Child Care Licensing, REPORT SUBMITTED BY, DATE, TO BE COMPLETED ONLY BY LICENSING, TELEPHONE NO, Date report received in Licensing, and EVALUATION OF SIR so that you can move on to the 3rd stage.
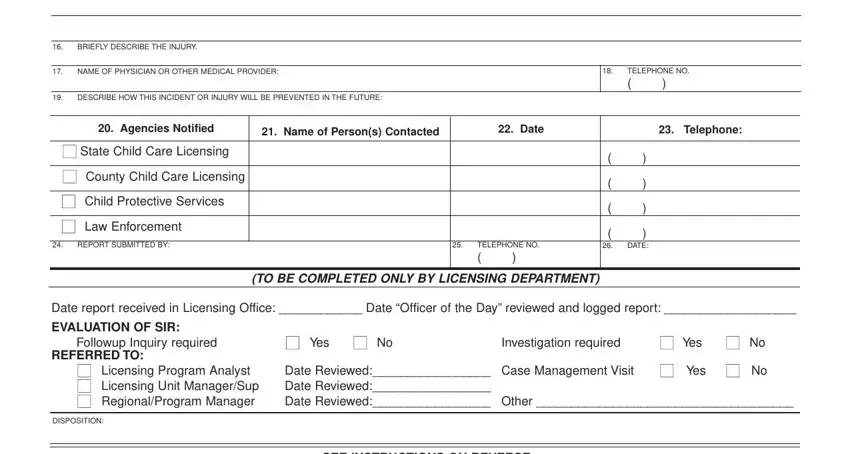
People who use this PDF generally make some mistakes while completing EVALUATION OF SIR in this area. Don't forget to read again whatever you enter here.
Step 3: Ensure that your information is accurate and simply click "Done" to progress further. After setting up a7-day free trial account here, you will be able to download TODAYS or send it through email promptly. The PDF file will also be accessible through your personal cabinet with all of your edits. FormsPal is dedicated to the privacy of all our users; we make certain that all personal data going through our system is protected.