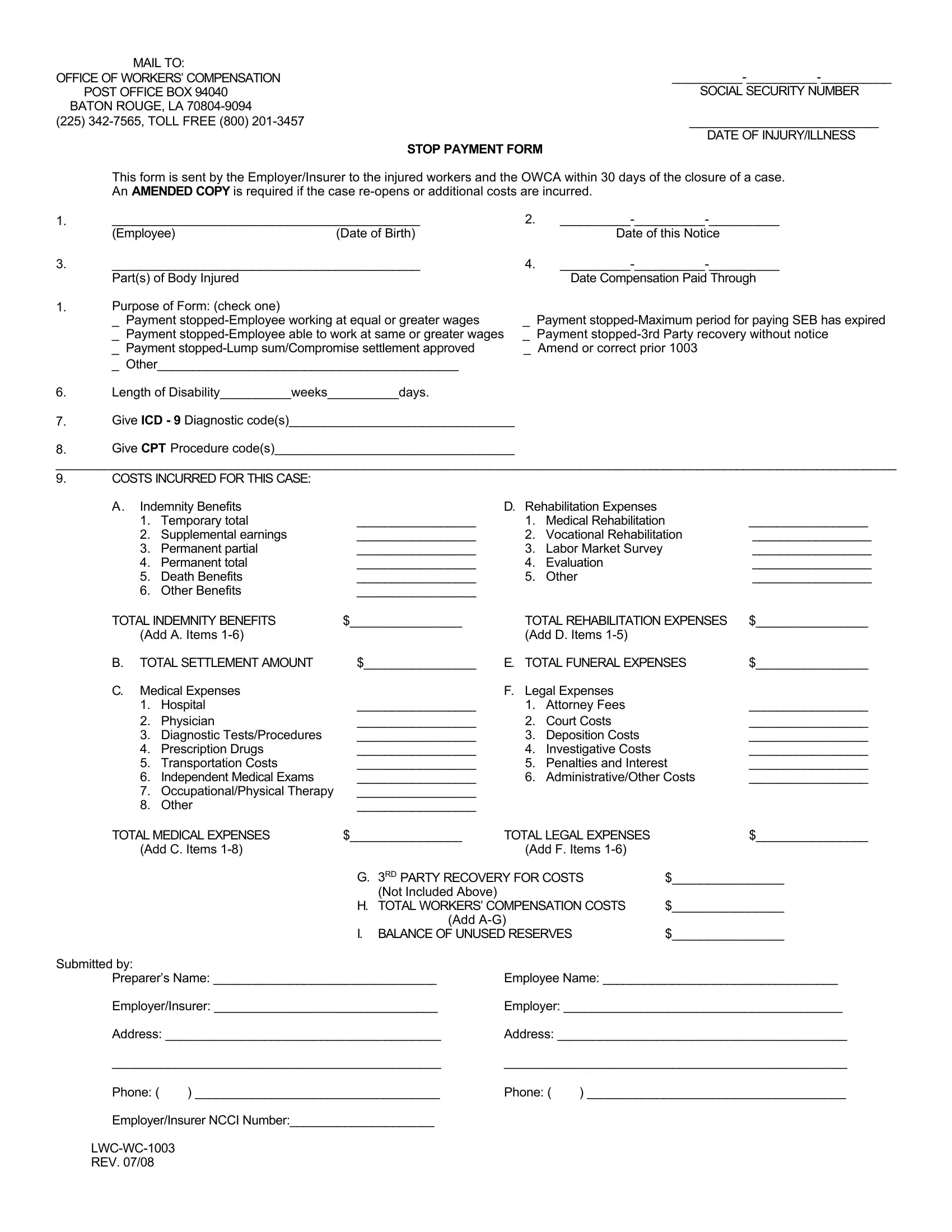
In the realm of workers' compensation, the intricacies of navigating post-injury procedures can be daunting for both employers and employees alike. The LWC WC 1003 Stop Payment form serves as a critical document in this process, ensuring that all parties are duly informed when an employer or insurer decides to terminate compensation payments to an injured worker. This form, mandated for use by the Office of Workers' Compensation in Baton Rouge, Louisiana, encapsulates a range of essential details, from the basics such as the worker's social security number and the injury date, to the specifics like the parts of the body injured and the compensation paid through date. Employers or insurers are required to furnish this document within 30 days of case closure, and an amended copy is necessary if the case re-opens or additional costs are incurred. The form also delineates the reasons for stopping payments—be it because the employee has returned to work at equal or greater wages, the maximum period for SEB payments has expired, a lump sum or compromise settlement has been approved, among other reasons. Beyond the cessation of payments, the form delves into the length of disability, diagnostic and procedure codes, incurred costs including indemnity benefits, rehabilitation expenses, medical expenses, and even funeral expenses when applicable, culminating in a comprehensive summary of the total workers’ compensation costs and the balance of unused reserves. This detailed framework not only ensures compliance with Louisiana's workers' compensation laws but also provides a structured means for tracking and managing the financial aspects of a worker's injury claim.
| Question | Answer |
|---|---|
| Form Name | Form Lwc Wc 1003 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | OWCA, Insurer, NCCI, LWC-WC-1003 |
|
MAIL TO: |
|
|
|
OFFICE OF WORKERS’ COMPENSATION |
|
|
||
|
POST OFFICE BOX 94040 |
|
|
SOCIAL SECURITY NUMBER |
|
BATON ROUGE, LA |
|
|
|
(225) |
|
|
___________________________ |
|
|
|
|
|
DATE OF INJURY/ILLNESS |
|
|
STOP PAYMENT FORM |
|
|
|
This form is sent by the Employer/Insurer to the injured workers and the OWCA within 30 days of the closure of a case. |
|||
|
An AMENDED COPY is required if the case |
|||
1. |
____________________________________________ |
2. |
||
|
(Employee) |
(Date of Birth) |
|
Date of this Notice |
3. |
____________________________________________ |
4. |
||
|
Part(s) of Body Injured |
|
|
Date Compensation Paid Through |
1.Purpose of Form: (check one)
_ Payment |
_ |
Payment |
|
_ |
Payment |
_ |
Payment |
_ |
Payment |
_ Amend or correct prior 1003 |
|
_ Other___________________________________________
6.Length of Disability__________weeks__________days.
7.Give ICD - 9 Diagnostic code(s)________________________________
8.Give CPT Procedure code(s)__________________________________
__________________________________________________________________________________________________________________________
9.COSTS INCURRED FOR THIS CASE:
A. Indemnity Benefits |
D. |
Rehabilitation Expenses |
|
||
1. |
Temporary total |
_________________ |
1. |
Medical Rehabilitation |
_________________ |
2. |
Supplemental earnings |
_________________ |
2. |
Vocational Rehabilitation |
_________________ |
3. |
Permanent partial |
_________________ |
3. |
Labor Market Survey |
_________________ |
4. |
Permanent total |
_________________ |
4. |
Evaluation |
_________________ |
5. |
Death Benefits |
_________________ |
5. |
Other |
_________________ |
6. |
Other Benefits |
_________________ |
|
|
|
TOTAL INDEMNITY BENEFITS |
$________________ |
TOTAL REHABILITATION EXPENSES |
$________________ |
|||
|
(Add A. Items |
|
(Add D. Items |
|
||
B. |
TOTAL SETTLEMENT AMOUNT |
$________________ |
E. TOTAL FUNERAL EXPENSES |
$________________ |
||
C. |
Medical Expenses |
|
F. Legal Expenses |
|
||
|
1. |
Hospital |
_________________ |
1. |
Attorney Fees |
_________________ |
|
2. |
Physician |
_________________ |
2. |
Court Costs |
_________________ |
|
3. |
Diagnostic Tests/Procedures |
_________________ |
3. |
Deposition Costs |
_________________ |
|
4. |
Prescription Drugs |
_________________ |
4. |
Investigative Costs |
_________________ |
|
5. |
Transportation Costs |
_________________ |
5. |
Penalties and Interest |
_________________ |
|
6. |
Independent Medical Exams |
_________________ |
6. |
Administrative/Other Costs |
_________________ |
|
7. |
Occupational/Physical Therapy |
_________________ |
|
|
|
|
8. |
Other |
_________________ |
|
|
|
TOTAL MEDICAL EXPENSES |
$________________ |
TOTAL LEGAL EXPENSES |
$________________ |
|||
(Add C. Items |
|
|
(Add F. Items |
|
||
|
|
G. |
3RD PARTY RECOVERY FOR COSTS |
$________________ |
||
|
|
|
(Not Included Above) |
|
|
|
|
|
H. TOTAL WORKERS’ COMPENSATION COSTS |
$________________ |
|||
|
|
|
(Add |
|
|
|
|
|
I. |
BALANCE OF UNUSED RESERVES |
|
$________________ |
|
Submitted by: |
|
|
|
|
|
|
Preparer’s Name: ________________________________ |
Employee Name: __________________________________ |
|||||
Employer/Insurer: ________________________________ |
Employer: ________________________________________ |
|||||
Address: _______________________________________ |
Address: _________________________________________ |
|||||
_______________________________________________ |
_________________________________________________ |
|||||
Phone: ( |
) ___________________________________ |
Phone: ( |
) _____________________________________ |
|||
Employer/Insurer NCCI Number:_____________________
REV. 07/08