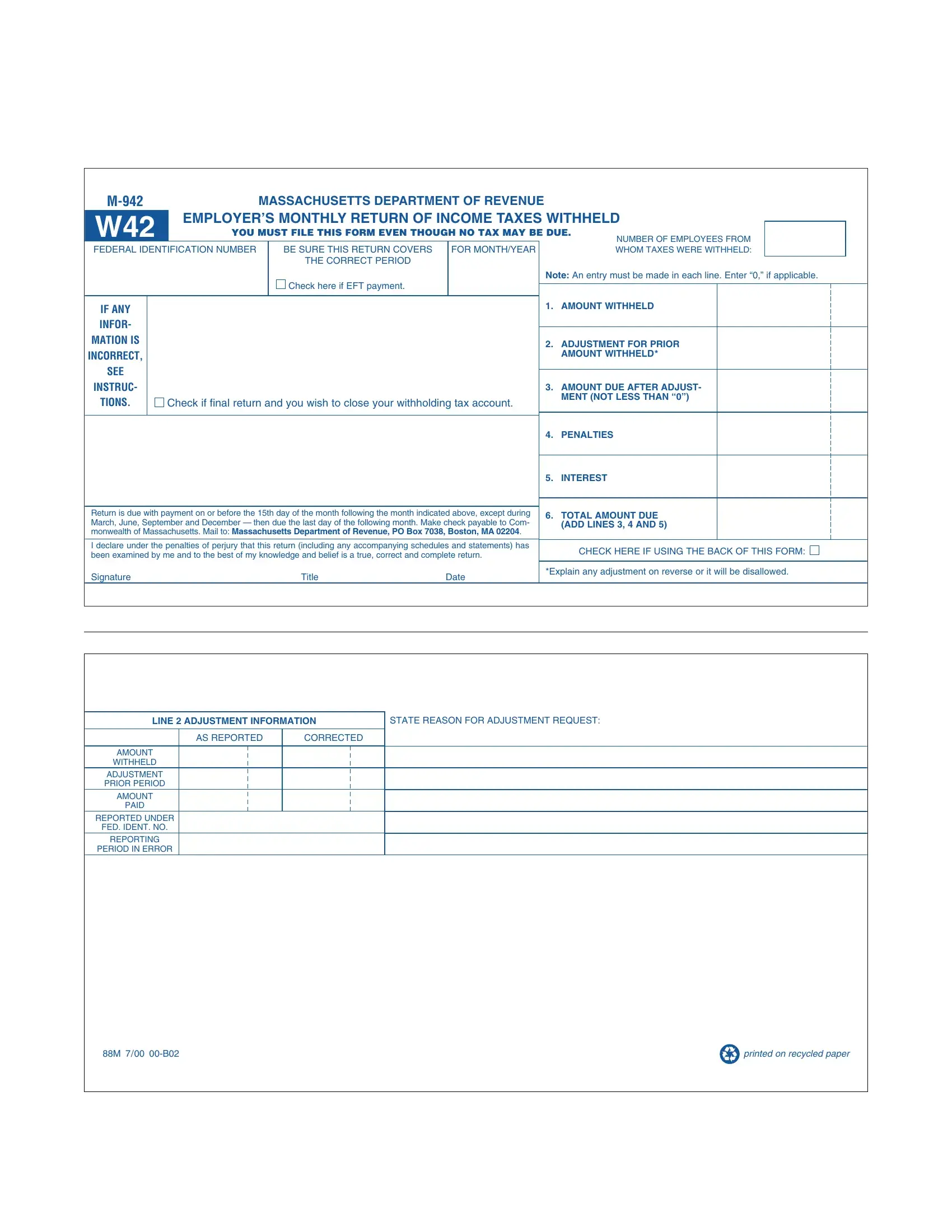
Navigating through the complexities of employee income tax withholding, employers in Massachusetts are acquainted with the M-942 form, a critical piece of documentation mandated by the Massachusetts Department of Revenue. This form, serving as the employer’s monthly return of income taxes withheld, enforces compliance even in instances where no tax is due. It demands meticulous attention to detail, from specifying the number of employees from whom taxes have been withheld to ensuring the accuracy of the business's federal identification number. Notably, the form incorporates sections for adjustments related to previous inaccuracies, penalties, and interest, thereby accommodating corrections that might affect the total amount due. With strict deadlines that vary according to the month, timely submission is crucial—by the 15th following most months, extending to the last day of the following month for quarterly intervals. The design of the form includes provisions for electronic funds transfer payments, and it aids businesses in concluding their withholding tax duties, should they mark it as a final return. By facilitating a direct communication channel with the state’s treasury through specified mailing instructions, the M-942 form stands as a testament to an employer’s adherence to state tax laws and their commitment to fiscal responsibility.
| Question | Answer |
|---|---|
| Form Name | Form M 942 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | m942 massachusetts, w42, massachusetts employer monthly, m 942 w42 |
|
MASSACHUSETTS DEPARTMENT OF REVENUE |
|
|
|
|
|
|||||||
W42 |
EMPLOYER’S MONTHLY RETURN OF INCOME TAXES WITHHELD |
|
|
||||||||||
YOU MUST FILE THIS FORM EVEN THOUGH NO TAX MAY BE DUE. |
|
|
|||||||||||
|
|
|
|
|
|
|
|
NUMBER OF EMPLOYEES FROM |
|
|
|||
FEDERAL IDENTIFICATION NUMBER |
|
BE SURE THIS RETURN COVERS |
|
FOR MONTH/YEAR |
|
|
WHOM TAXES WERE WITHHELD: |
|
|
||||
|
|
|
|
THE CORRECT PERIOD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Note: An entry must be made in each line. Enter “0,” if applicable. |
||||
|
|
|
|
Check here if EFT payment. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BUSINESS |
NAME |
|
|
|
|
|
|
1. |
AMOUNT WITHHELD |
|
|
|
|
IF ANY |
|
|
|
|
|
|
|
|
|
|
|
||
INFOR- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
MATIONBUS NESSIS |
ADDRESS |
|
|
|
|
|
|
2. |
ADJUSTMENT FOR PRIOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
INCORRECT, |
|
|
|
|
|
|
|
|
|
AMOUNT WITHHELD* |
|
|
|
SEE |
|
|
|
STATE |
ZIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
CITY/TOWN |
|
|
|
|
|
|
|
|
|
|
|
||
INSTRUC- |
|
|
|
|
|
|
|
|
3. |
AMOUNT DUE AFTER ADJUST- |
|
|
|
TIONS. |
|
Check if final return and you wish to close your withholding tax account. |
|
|
MENT (NOT LESS THAN “0”) |
|
|
|
|||||
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
PENALTIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
INTEREST |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Return is due with payment on or before the 15th day of the month following the month indicated above, except during |
|
6. |
TOTAL AMOUNT DUE |
|
|
|
|||||||
March, June, September and December — then due the last day of the following month. Make check payable to Com- |
|
|
|
|
|||||||||
|
|
(ADD LINES 3, 4 AND 5) |
|
|
|
||||||||
monwealth of Massachusetts. Mail to: Massachusetts Department of Revenue, PO Box 7038, Boston, MA 02204. |
|
|
|
|
|
||||||||
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|||||
I declare under the penalties of perjury that this return (including any accompanying schedules and statements) has |
|
|
CHECK HERE IF USING THE BACK OF THIS FORM: |
||||||||||
been examined by me and to the best of my knowledge and belief is a true, correct and complete return. |
|
|
|||||||||||
|
|
|
|
|
|
||||||||
Signature |
|
|
Title |
|
Date |
|
*Explain any adjustment on reverse or it will be disallowed. |
||||||
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LINE 2 ADJUSTMENT INFORMATION |
STATE REASON FOR ADJUSTMENT REQUEST: |
|
AS REPORTED |
CORRECTED |
|
AMOUNT |
|
|
WITHHELD |
|
|
ADJUSTMENT |
|
|
PRIOR PERIOD |
|
|
AMOUNT |
|
|
PAID |
|
|
REPORTED UNDER |
|
|
FED. IDENT. NO. |
|
|
REPORTING |
|
|
PERIOD IN ERROR |
|
|
88M 7/00 |
|
printed on recycled paper |