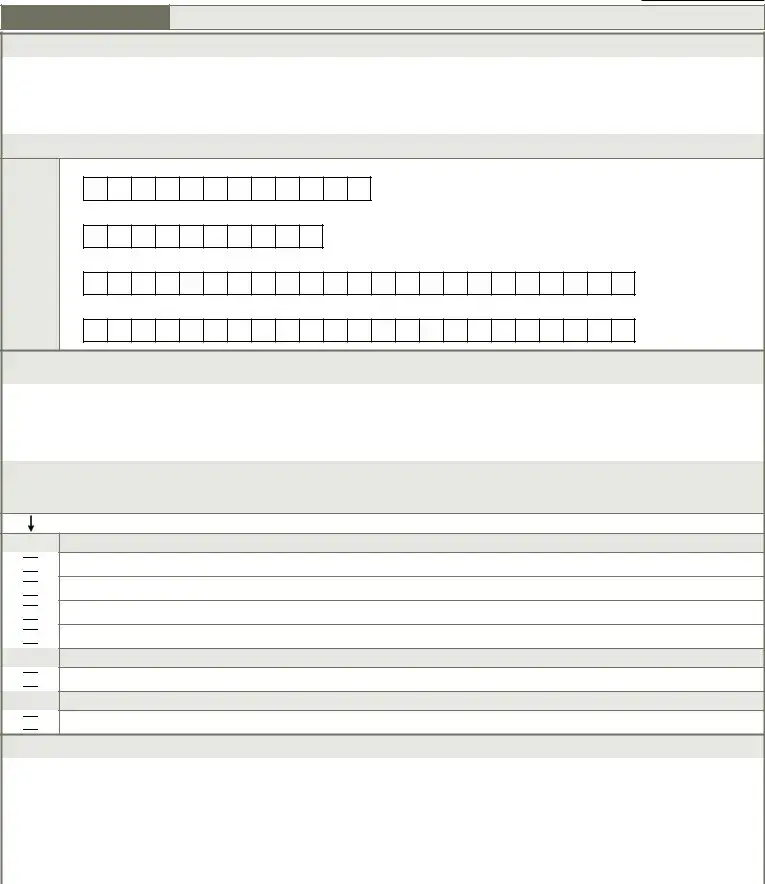
 A. Down syndrome
A. Down syndrome B. Autism
B. Autism C. Epilepsy
C. Epilepsy D. Other organic condition related to MR/DD
D. Other organic condition related to MR/DD E. MR/DD with no organic condition
E. MR/DD with no organic condition Z. None of the above
Z. None of the above
 Skip to B0100, Comatose
Skip to B0100, Comatose Continue to A2400B, Start date of most recent Medicare stay
Continue to A2400B, Start date of most recent Medicare stay
 Continue to B0200, Hearing
Continue to B0200, Hearing Skip to G0110, Activities of Daily Living (ADL) Assistance
Skip to G0110, Activities of Daily Living (ADL) AssistanceIt shouldn’t be difficult to create blank mds 3 0 2020 applying our PDF editor. This is the way you may effortlessly prepare your document.
Step 1: Choose the button "Get Form Here".
Step 2: You can now change your blank mds 3 0 2020. The multifunctional toolbar will allow you to insert, remove, modify, and highlight content material or perform other sorts of commands.
Provide the details required by the platform to fill in the form.
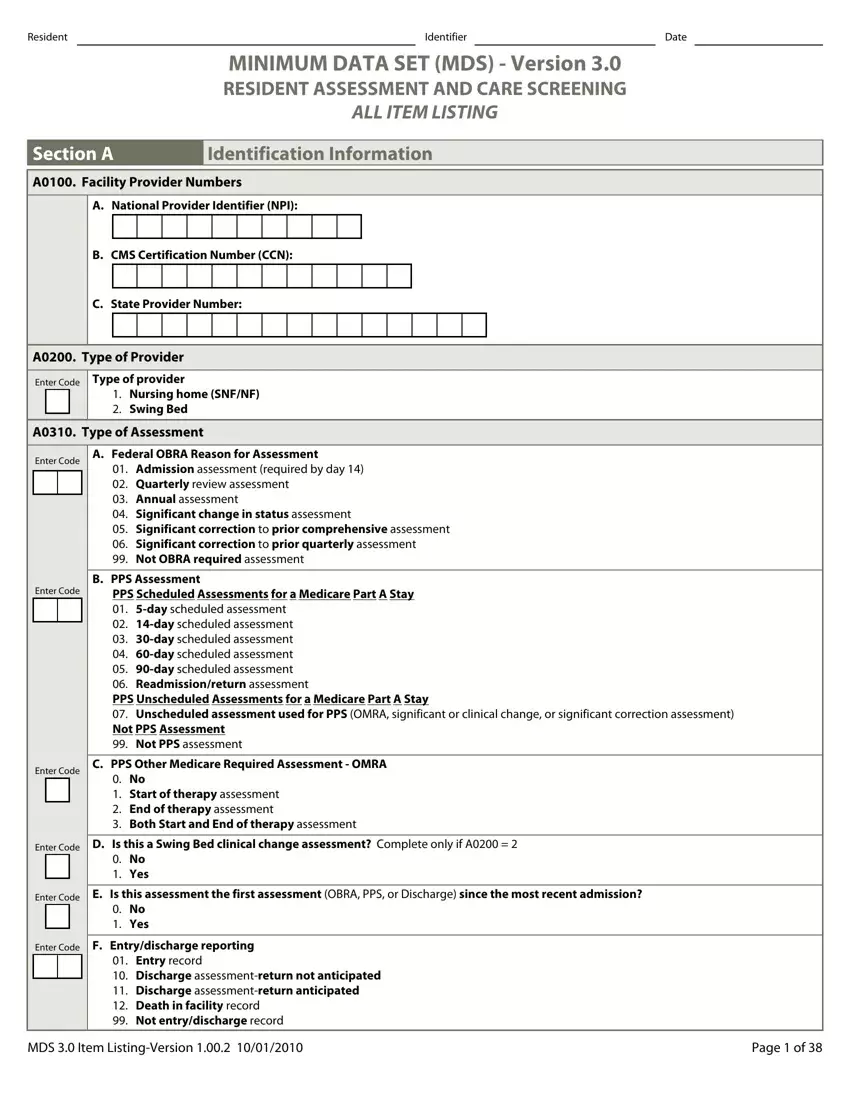
Provide the requested data in the box Enter Code, Enter Code, A Federal OBRA Reason for, Admission assessment required by, B PPS Assessment, PPS Scheduled Assessments for a, Enter Code, C PPS Other Medicare Required, No Start of therapy assessment, Enter Code, D Is this a Swing Bed clinical, No Yes, Enter Code, E Is this assessment the first, and No Yes.
The system will require you to give certain key data to instantly fill out the area Enter Code, F Entrydischarge reporting, Entry record Discharge, MDS Item ListingVersion, and Page of.

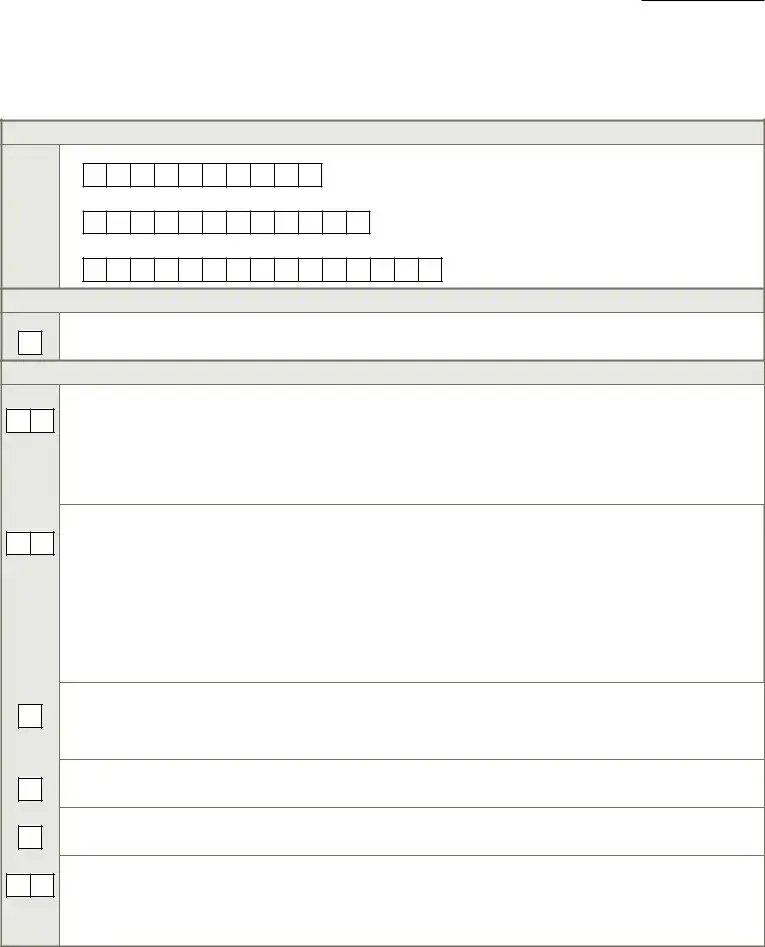
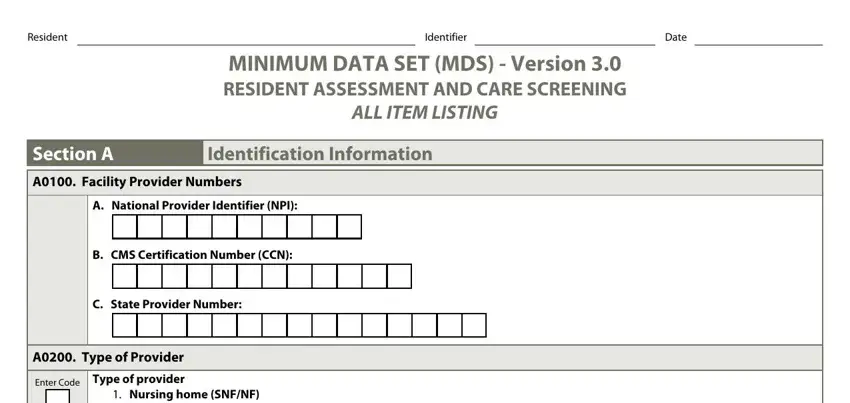
The Resident, Identifier, Date, Section A, Identification Information, A Submission Requirement, Enter Code, Neither federal nor state, A Legal Name of Resident, A First name, C Last name, B Middle initial, D Suffix, A Social Security and Medicare, and A Social Security Number field has to be used to provide the rights or obligations of each party.
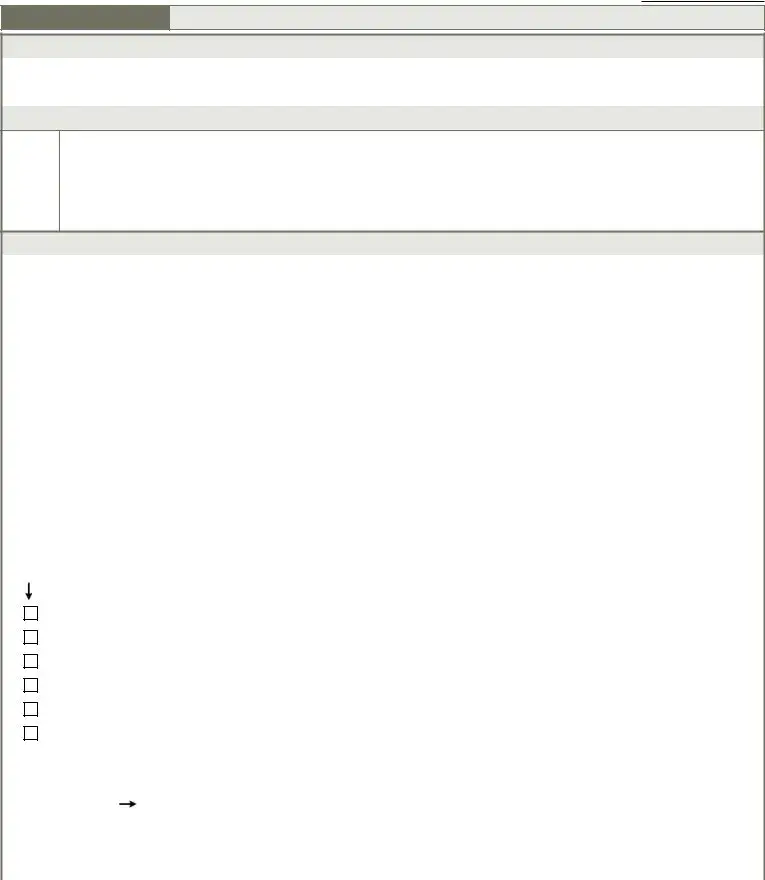
Prepare the document by analyzing the next sections: A Medicaid Number Enter if, A Gender, Enter Code, Male Female, A Birth Date, Month, Day, Year, A RaceEthnicity, Check all that apply, A American Indian or Alaska Native, B Asian, C Black or African American, D Hispanic or Latino, and E Native Hawaiian or Other Pacific.
Step 3: Choose the Done button to save the form. Then it is obtainable for upload to your gadget.
Step 4: Generate duplicates of your form - it can help you stay clear of upcoming difficulties. And don't be concerned - we don't reveal or check your data.
