Bryn Mawr Hospital |
Lankenau Hospital |
Paoli Hospital |
Bryn Mawr Rehabilitation |
130 South Bryn Mawr Avenue |
100 Lancaster Avenue |
255 West Lancaster Avenue |
414 Paoli Pike |
Bryn Mawr, PA 19010 |
Wynnewood, PA 19096 |
Paoli, PA 19301 |
Malvern, PA 19355 |
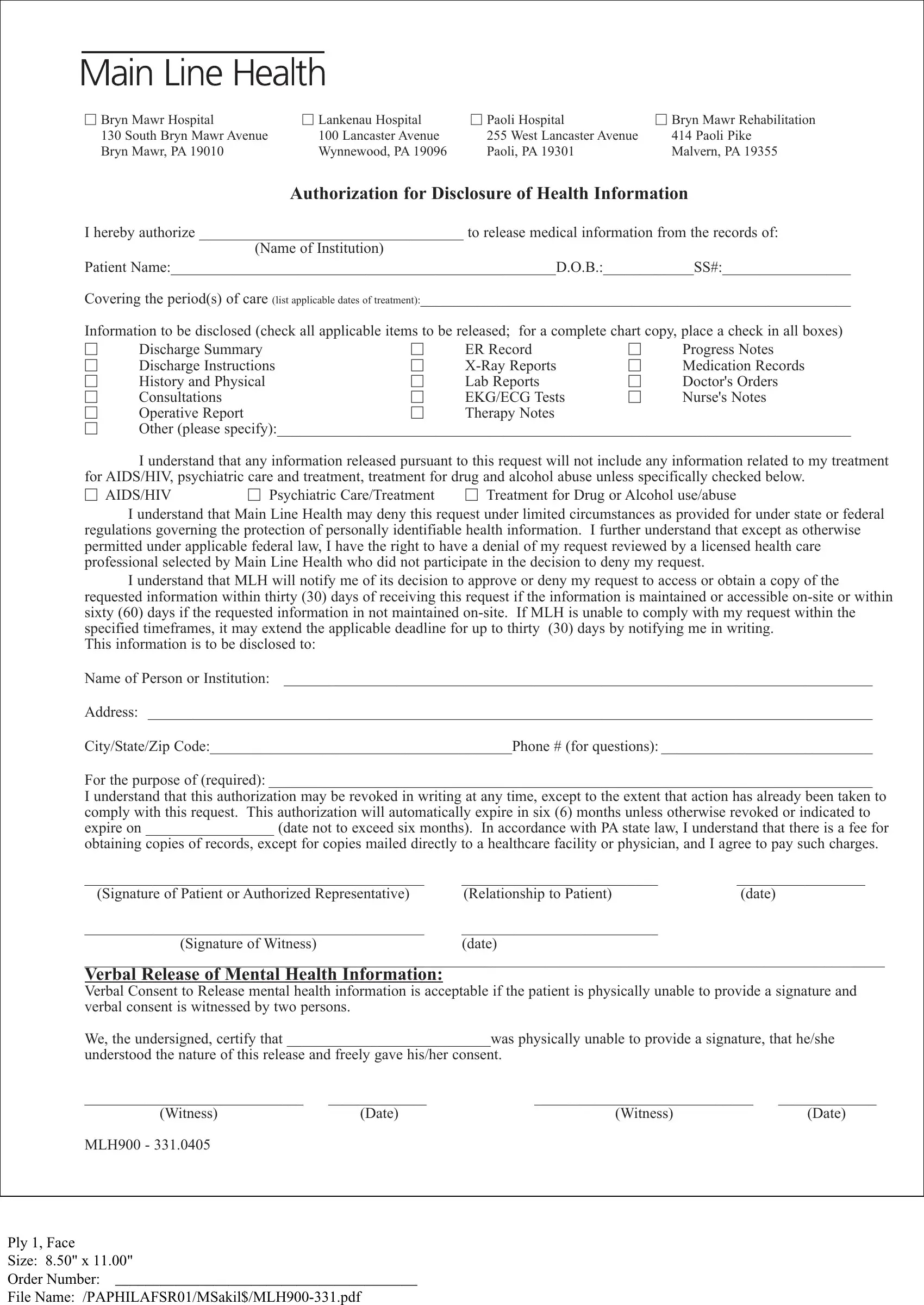
AUTHORIZATION FOR DISCLOSURE OF HEALTH INFORMATION
I hereby authorize ___________________________________ to release medical information from the records of:
(Name of Institution)
Patient Name:___________________________________________________D.O.B.:____________SS#:_________________
Covering the period(s) of care (list applicable dates of treatment):_________________________________________________________
Information to be disclosed (check all applicable items to be released; for a complete chart copy, place a check in all boxes)
|
Discharge Summary |
|
ER Record |
|
Progress Notes |
|
Discharge Instructions |
|
X-Ray Reports |
|
Medication Records |
|
History and Physical |
|
Lab Reports |
|
Doctor's Orders |
|
Consultations |
|
EKG/ECG Tests |
|
Nurse's Notes |
|
Operative Report |
|
Therapy Notes |
|
|
Other (please specify):____________________________________________________________________________
I understand that any information released pursuant to this request will not include any information related to my treatment for AIDS/HIV, psychiatric care and treatment, treatment for drug and alcohol abuse unless specifically checked below.
AIDS/HIV |
Psychiatric Care/Treatment |
Treatment for Drug or Alcohol use/abuse |
I understand that Main Line Health may deny this request under limited circumstances as provided for under state or federal regulations governing the protection of personally identifiable health information. I further understand that except as otherwise permitted under applicable federal law, I have the right to have a denial of my request reviewed by a licensed health care professional selected by Main Line Health who did not participate in the decision to deny my request.
I understand that MLH will notify me of its decision to approve or deny my request to access or obtain a copy of the requested information within thirty (30) days of receiving this request if the information is maintained or accessible on-site or within sixty (60) days if the requested information in not maintained on-site. If MLH is unable to comply with my request within the specified timeframes, it may extend the applicable deadline for up to thirty (30) days by notifying me in writing.
This information is to be disclosed to:
Name of Person or Institution: ______________________________________________________________________________
Address: ________________________________________________________________________________________________
City/State/Zip Code:________________________________________Phone # (for questions): ____________________________
For the purpose of (required): ________________________________________________________________________________
I understand that this authorization may be revoked in writing at any time, except to the extent that action has already been taken to comply with this request. This authorization will automatically expire in six (6) months unless otherwise revoked or indicated to expire on _________________ (date not to exceed six months). In accordance with PA state law, I understand that there is a fee for
obtaining copies of records, except for copies mailed directly to a healthcare facility or physician, and I agree to pay such charges.
_____________________________________________ |
__________________________ |
_________________ |
(Signature of Patient or Authorized Representative) |
(Relationship to Patient) |
(date) |
_____________________________________________ |
__________________________ |
|
(Signature of Witness) |
(date) |
|
__________________________________________________________________________________________________________
VERBAL RELEASE OF MENTAL HEALTH INFORMATION:
Verbal Consent to Release mental health information is acceptable if the patient is physically unable to provide a signature and verbal consent is witnessed by two persons.
We, the undersigned, certify that ___________________________was physically unable to provide a signature, that he/she
understood the nature of this release and freely gave his/her consent.
_____________________________ |
_____________ |
_____________________________ |
_____________ |
(Witness) |
(Date) |
(Witness) |
(Date) |
MLH900 - 331.0405 |
|
|
|
Ply 1, Face
Size: 8.50" x 11.00"
Order Number: ________________________________________
File Name: /PAPHILAFSR01/MSakil$/MLH900-331.pdf
INSTRUCTIONS FOR COMPLETING THE
AUTHORIZATION FOR DISCLOSURE OF HEALTH INFORMATION FORM
1.Please complete the Authorization for Disclosure of Health Information Form in its entirety. Incomplete forms will be returned to the sender for completion.
2.The patient or legally authorized representative (see #7 below) must sign and date the form.
3.Please mail the form to the appropriate facility to the attention of the "Health Information Management Department." The address for each hospital is listed at the top of the authorization form. Electronic copies will not be accepted.
4.Records will be mailed directly to the party listed as the recipient on the authorization form. We do not fax records to recipients unless needed for emergent patient care by another healthcare provider.
5.If the records are needed for continuing care purposes and are mailed directly to a physician or other healthcare facility, the records will be provided free of charge.
6.Records for all other purposes are subject to copying charges in accordance with PA State Law. An invoice will be mailed to you and payment will be expected prior to the records being copied and mailed.
7.The following is a list of persons authorized to sign the disclosure of health information form:
•If the patient is 18 years of age or older and is competent, then the patient must sign. No one else is authorized to sign.
•If the patient is 14 years of age or older and was treated for a psychiatric admission, then the patient must sign.
•If the patient is a minor (under 18 years of age) or under 14 years of age for psychiatric admission, then the parent or legal guardian must sign.
•If the patient is over 18 years of age and is incompetent, then the legal representative must sign and provide proof of legal representation. (e.g. a photocopy of power of attorney documents or other legal documents).
•If the patient is deceased, the surviving spouse or other legal representative must sign and provide proof of legal representation (e.g. a photocopy of executor documentation, power of attorney, etc.).
Please contact the Health Information Management Department (Medical Records) at the appropriate facility if you have additional questions or need further assistance.
MLH900 -331.0405
Ply 1, Back
Size: 8.50" x 11.00"
Order Number: ________________________________________
File Name: /PAPHILAFSR01/MSakil$/MLH900-331.pdf