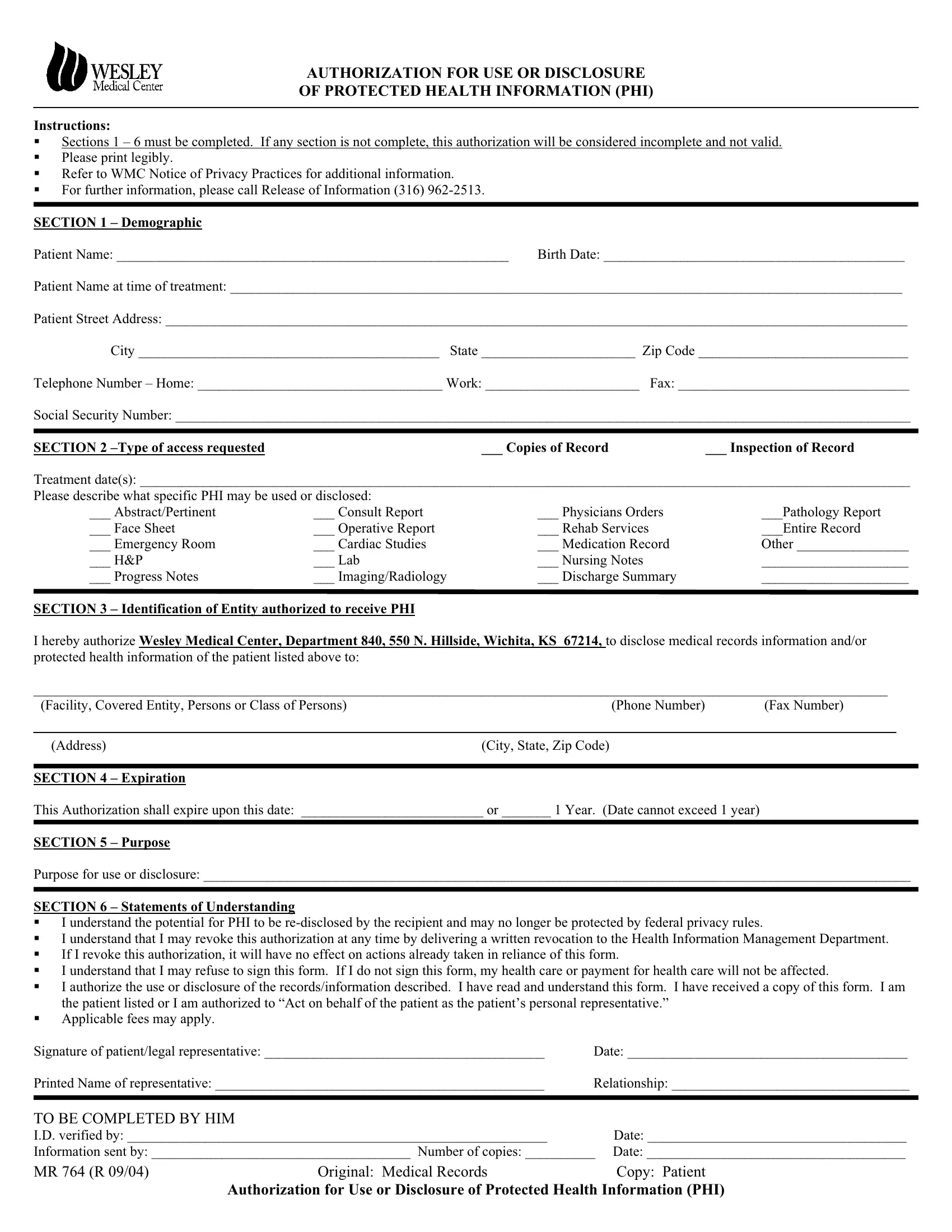
AUTHORIZATION FOR USE OR DISCLOSURE
OF PROTECTED HEALTH INFORMATION (PHI)
Instructions:
Sections 1 – 6 must be completed. If any section is not complete, this authorization will be considered incomplete and not valid.
Please print legibly.
Refer to WMC Notice of Privacy Practices for additional information.
For further information, please call Release of Information (316) 962-2513.
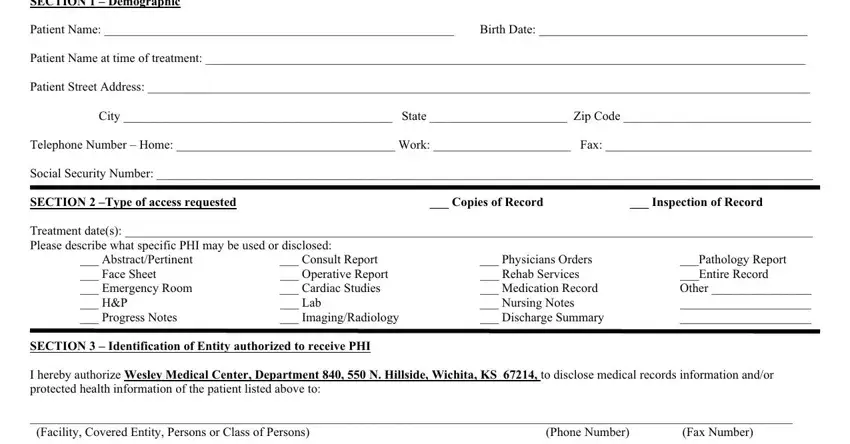
SECTION 1 – Demographic
Patient Name: ________________________________________________________ Birth Date: ___________________________________________
Patient Name at time of treatment: ________________________________________________________________________________________________
Patient Street Address: __________________________________________________________________________________________________________
City ___________________________________________ State ______________________ Zip Code ______________________________
Telephone Number – Home: ___________________________________ Work: ______________________ Fax: _________________________________
Social Security Number: _________________________________________________________________________________________________________
SECTION 2 –Type of access requested___ Copies of Record ___ Inspection of Record
Treatment date(s): ______________________________________________________________________________________________________________
Please describe what specific PHI may be used or disclosed:
___ Abstract/Pertinent |
___ Consult Report |
___ Physicians Orders |
___Pathology Report |
___ Face Sheet |
___ Operative Report |
___ Rehab Services |
___Entire Record |
___ Emergency Room |
___ Cardiac Studies |
___ Medication Record |
Other ________________ |
___ H&P |
___ Lab |
___ Nursing Notes |
_____________________ |
___ Progress Notes |
___ Imaging/Radiology |
___ Discharge Summary |
_____________________ |
SECTION 3 – Identification of Entity authorized to receive PHI
I hereby authorize Wesley Medical Center, Department 840, 550 N. Hillside, Wichita, KS 67214, to disclose medical records information and/or protected health information of the patient listed above to:
__________________________________________________________________________________________________________________________
(Facility, Covered Entity, Persons or Class of Persons) |
(Phone Number) |
(Fax Number) |
|
|
|
|
(Address) |
|
(City, State, Zip Code) |
|
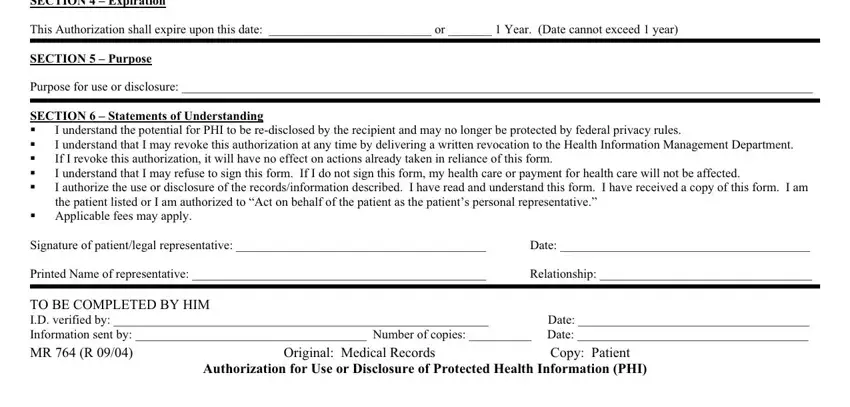
SECTION 4 |
– Expiration |
|
|
This Authorization shall expire upon this date: __________________________ or _______ 1 Year. (Date cannot exceed 1 year) |
|
SECTION 5 |
– Purpose |
|
|
Purpose for use or disclosure: _____________________________________________________________________________________________________
SECTION 6 – Statements of Understanding
I understand the potential for PHI to be re-disclosed by the recipient and may no longer be protected by federal privacy rules.
I understand that I may revoke this authorization at any time by delivering a written revocation to the Health Information Management Department.
If I revoke this authorization, it will have no effect on actions already taken in reliance of this form.
I understand that I may refuse to sign this form. If I do not sign this form, my health care or payment for health care will not be affected.
I authorize the use or disclosure of the records/information described. I have read and understand this form. I have received a copy of this form. I am the patient listed or I am authorized to “Act on behalf of the patient as the patient’s personal representative.”
Applicable fees may apply.
Signature of patient/legal representative: ________________________________________ |
Date: ________________________________________ |
Printed Name of representative: _______________________________________________ |
Relationship: __________________________________ |
TO BE COMPLETED BY HIM
I.D. verified by: ____________________________________________________________ |
Date: _____________________________________ |
Information sent by: _____________________________________ Number of copies: __________ |
Date: _____________________________________ |
MR 764 (R 09/04) |
Original: Medical Records |
Copy: Patient |
Authorization for Use or Disclosure of Protected Health Information (PHI)