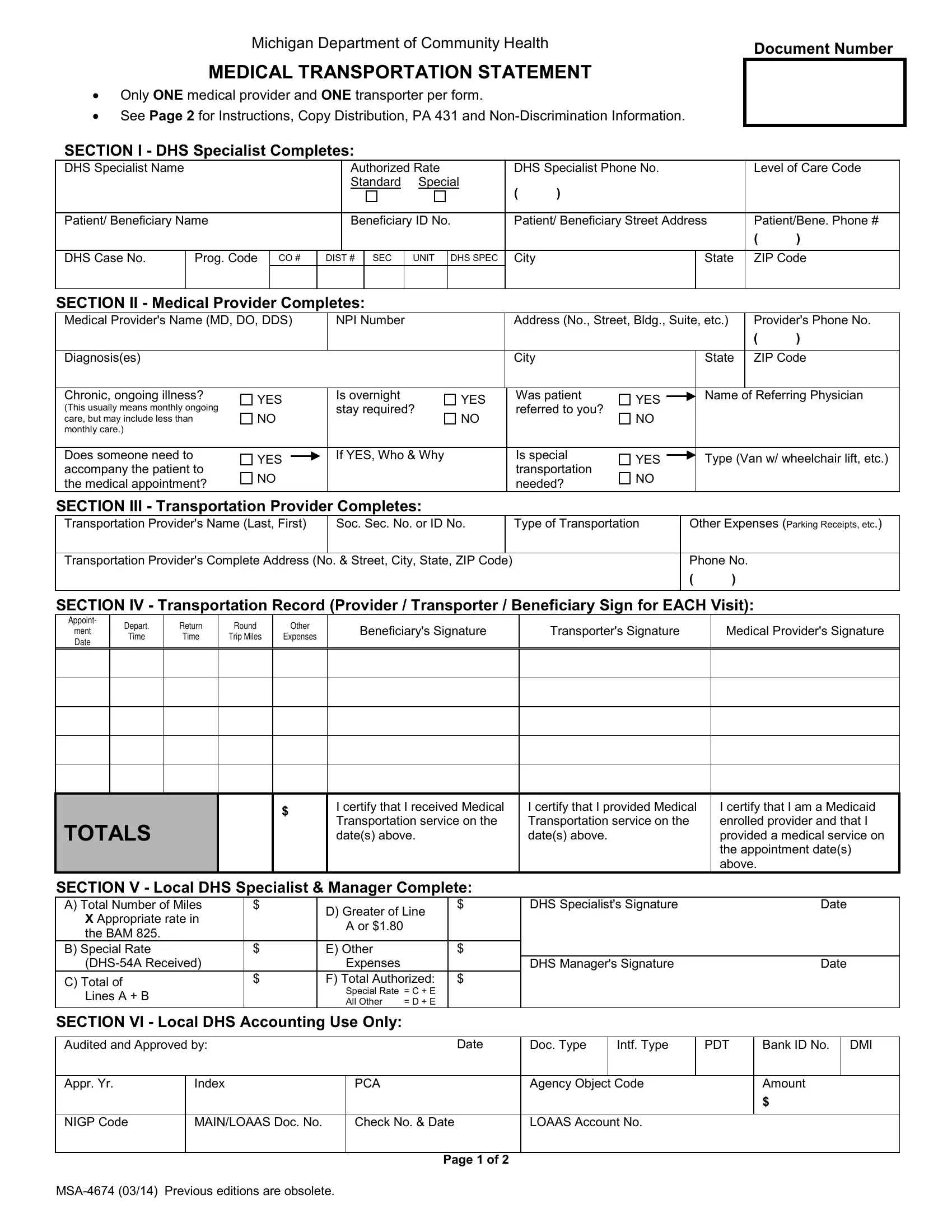
The MSA-4674 form, a crucial document administered by the Michigan Department of Community Health, serves as a standardized method for accounting medical transportation services rendered to beneficiaries, ensuring a seamless process for both medical providers and transporters to claim their services. Tailored specifically to capture instances where only one medical provider and transporter are involved per form, the document demands meticulous completion to facilitate the authorization and payment for medical transportation needs. Given its structured layout, the form aids in streamlining the submission and review of such transportation claims, with distinct sections designated for completion by different stakeholders including DHS Specialists, medical providers, transportation providers, and beneficiaries themselves. The form encompasses details on the service provided - such as diagnosis, type of transportation required, and appointment records - while also outlining instructions for its use, copy distribution, and the critical importance of timely submission within 90 calendar days from the service date. With provisions for documenting each transportation event and a detailed breakdown of incurred costs, the MSA-4674 is instrumental in ensuring accurate reimbursement for transportation services essential for beneficiaries’ medical care, emphasizing the complex interplay between healthcare accessibility and administrative processes.
| Question | Answer |
|---|---|
| Form Name | Form Msa 4674 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | PCA, DHS, PDT, Intf |