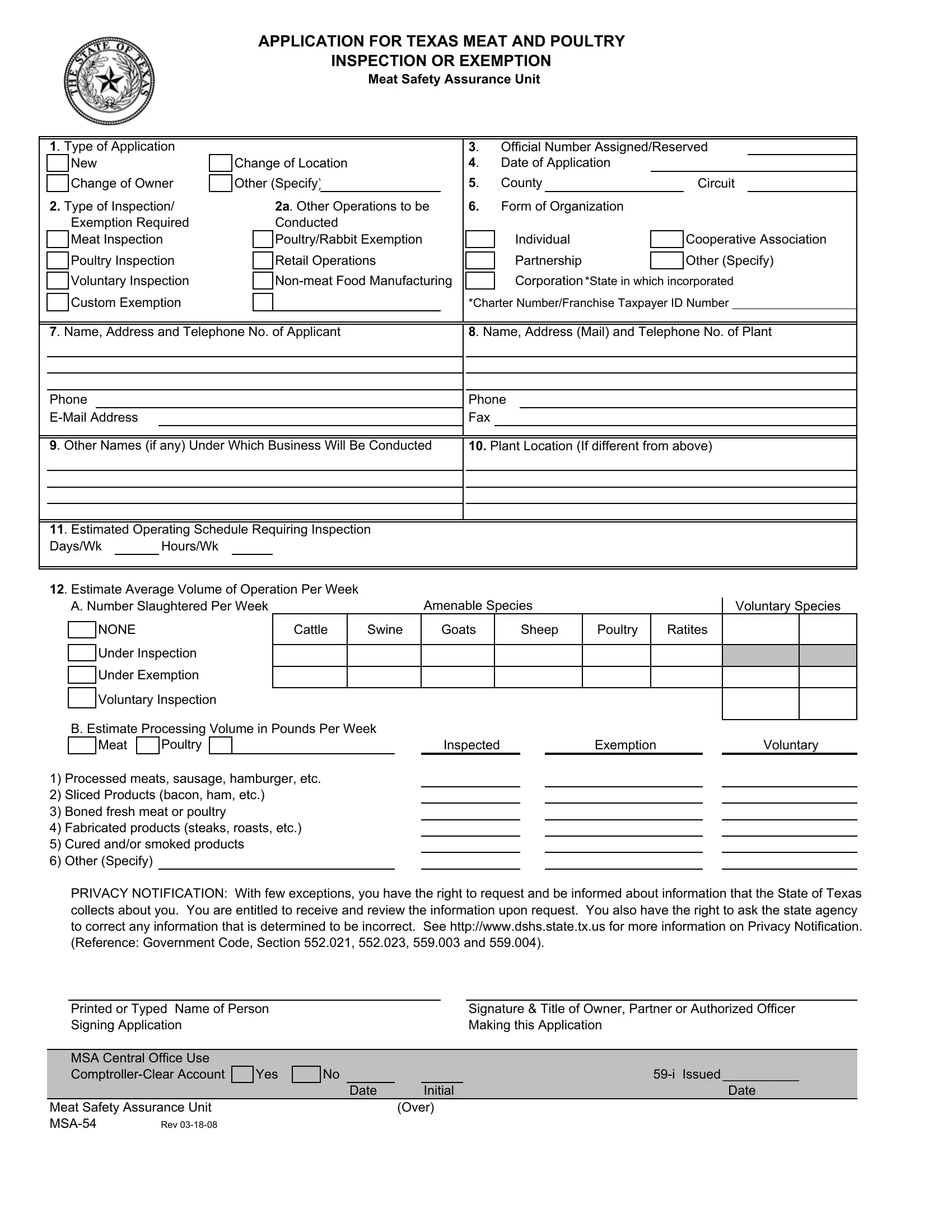
Navigating the complex requirements of the Texas meat and poultry inspection or exemption process is crucial for businesses in the industry, and the MSA 54 form serves as a vital starting point. This comprehensive form, issued by the Texas Department of State Health Services, is designed for applicants seeking either inspection services or exemption status under state regulations. It covers a broad range of details, including type of application, inspection and exemption types, business organization form, and a detailed account of operational aspects like location, estimated volume, and operational schedules. Additionally, it requests information on the ownership and management of the applying entity, including any criminal convictions related to food handling or fraud. The form also underlines the commitment applicants must make to adhere to the strict regulations governing meat and poultry safety, underscoring the legal and ethical responsibilities of businesses within the industry. With sections dedicated to privacy rights and non-discrimination policies, the MSA 54 form exemplifies the state's commitment to both consumer safety and applicant fairness. Completing and submitting this form is the first step for businesses to ensure compliance with Texas health and safety codes, ultimately aiming to protect public health while supporting industry operations.
| Question | Answer |
|---|---|
| Form Name | Form Msa 54 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 59-i, SERIVCES, 1872, TEXAS |
APPLICATION FOR TEXAS MEAT AND POULTRY
INSPECTION OR EXEMPTION
Meat Safety Assurance Unit
|
1. Type of Application |
|
|
|
|
|
|
|
|
|
|
3. |
|
Official Number Assigned/Reserved |
||||||||||||||||||
|
|
New |
|
|
Change of Location |
|
|
|
|
4. |
|
Date of Application |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
County |
|
|
|
|
|
|
|
|
|
|||
|
|
Change of Owner |
|
Other (Specify) |
|
|
|
|
|
|
|
|
|
Circuit |
|
|||||||||||||||||
|
2. Type of Inspection/ |
|
|
|
2a. Other Operations to be |
|
6. |
|
Form of Organization |
|
|
|
|
|
|
|
||||||||||||||||
|
|
Exemption Required |
|
|
|
Conducted |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
Meat Inspection |
|
|
|
Poultry/Rabbit Exemption |
|
|
|
Individual |
|
|
|
Cooperative Association |
||||||||||||||||||
|
|
Poultry Inspection |
|
|
|
Retail Operations |
|
|
|
Partnership |
|
|
|
Other (Specify) |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
Voluntary Inspection |
|
|
|
|
|
Corporation*State in which incorporated |
||||||||||||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
Custom Exemption |
|
|
|
|
|
|
|
|
|
|
*Charter Number/Franchise Taxpayer ID Number |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
7. Name, Address and Telephone No. of Applicant |
|
|
|
|
8. Name, Address (Mail) and Telephone No. of Plant |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
9. Other Names (if any) Under Which Business Will Be Conducted |
|
10. Plant Location (If different from above) |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
11. Estimated Operating Schedule Requiring Inspection |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Days/Wk |
|
Hours/Wk |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Estimate Average Volume of Operation Per Week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
A. Number Slaughtered Per Week |
|
|
Amenable Species |
|
|
|
|
|
|
Voluntary Species |
||||||||||||||||||||
|
|
|
NONE |
|
|
|
|
|
Cattle |
|
Swine |
|
Goats |
|
|
|
Sheep |
Poultry |
|
Ratites |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
Under Inspection |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
Under Exemption |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Voluntary Inspection |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
B. Estimate Processing Volume in Pounds Per Week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
Meat |
|
Poultry |
|
|
|
|
|
|
|
|
|
|
Inspected |
|
|
|
|
Exemption |
|
|
|
|
|
Voluntary |
|||||
1)Processed meats, sausage, hamburger, etc.
2)Sliced Products (bacon, ham, etc.)
3)Boned fresh meat or poultry
4)Fabricated products (steaks, roasts, etc.)
5)Cured and/or smoked products
6)Other (Specify)
PRIVACY NOTIFICATION: With few exceptions, you have the right to request and be informed about information that the State of Texas collects about you. You are entitled to receive and review the information upon request. You also have the right to ask the state agency to correct any information that is determined to be incorrect. See http://www.dshs.state.tx.us for more information on Privacy Notification. (Reference: Government Code, Section 552.021, 552.023, 559.003 and 559.004).
Printed or Typed Name of Person Signing Application
Signature & Title of Owner, Partner or Authorized Officer Making this Application
MSA Central Office Use |
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
|
||||
|
|
|
|
|
|
Date |
|
Initial |
Date |
Meat Safety Assurance Unit |
|
|
|
|
|
(Over) |
|
||
Rev |
|
|
|
|
|
|
|
|
|
13.List all persons responsible connected with applicant Include all partners,officers, and owners of 10 percent more of voting stock, and employees in a managerial or executive capacity in the business. Notify the Regional MSA Program Manager of any changes in the listing
(ATTACH ADDENDUM IF MORE SPACE IS NEEDED)
|
Address (Include Zip Code) |
10% Or More Stock holder (if |
||
Name |
|
|
incorporated) |
|
Title |
|
Yes (X) |
|
No (X) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. Enter the name of each person listed under Item 13 who has been convicted in any Federal or State court of any felony. Enter the name of each person listed under Item 13 who has been convicted in any Federal or State court of more than one violation of any law, other than a felony, based upon the acquiring, handling,or distributing of unwholesome, mislabeled, or deceptively packaged food or upon fraud in connection with transactions in food. Include the nature of the crime, the date of conviction and the court in which convicted. If None, write "NONE."
15. List each conviction against the applicant (person, firm, or corporation) in any Federal or State court of any felony. List each conviction against the applicant (person, firm, or corporation) in any Federal or State court of more than one violationof any law other than a felony, based upon the acquiring, handling, or distributing of unwholesome, mislabeled, or deceptively packaged food or upon fraud in connection with
transactions in food. Include the nature of the crime, the date of conviction and the court in which convicted. If None, write |
NONE" |
." |
AGREEMENT AND CERTIFICATION:If inspection or exemption is granted under this registration, I (we) expressly agree to conform strictly to Chapter 433 of the Health and Safety Code, the Regulations governing Meat Inspection (9CFR Part 301 et seq.) , and the applicable rules adopted by the Texas Department State Health Services. I CERTIFY that all statements made herein are true to the best of my knowledge.
In accordance with Federal law and U.S. Department of Agriculture policy, this institutionis prohibited from discriminatingon the basis of race, color, national origin, sex, religion, age, or disability. To file a complaint of discrimination,contact the U.S. Department of Agriculture,Director, Office of Adjudication and Compliance, 1400 Independence Avenue S.W., Washington, D.C.
(202)
Printed or Typed Name of Person |
Signature & Title of Owner, Partner or Authorized Officer |
Signing Application |
Making this Application |
TO BE COMPLETED BY MEAT SAFETY ASSURANCE UNIT
Return Completed Application to: TEXAS DEPARTMENT OF STATE HEALTH SERIVCES
MEAT SAFETY ASSURANCE UNIT - Mail Code 1872
P.O. Box 149347
AUSTIN, TEXAS
Date Approved |
Signature of Director, MSA |
This establishment to be under Texas Meat & Poultry Inspection Act
Meat Safety Assurance Unit