Very few things are simpler than completing documentation using our PDF editor. There is not much you should do to enhance the nf 6 employer's wage verification form document - only adopt these measures in the following order:
Step 1: Hit the button "Get form here" to access it.
Step 2: The form editing page is now open. You can include text or enhance present content.
The following parts are inside the PDF form you'll be completing.
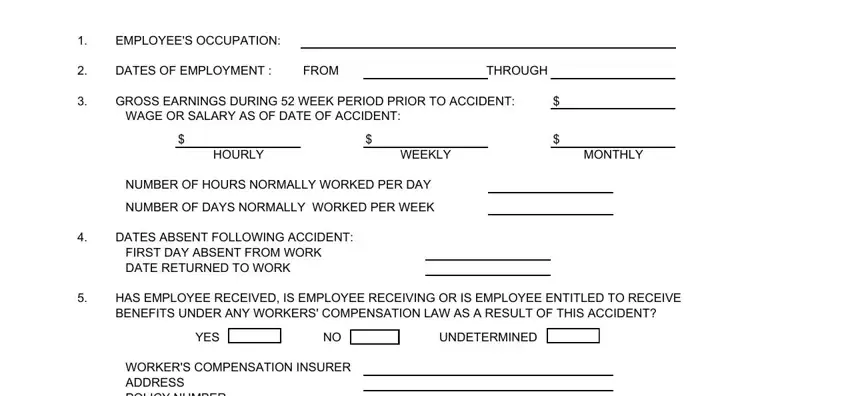
The program will need you to submit the EMPLOYEES OCCUPATION, DATES OF EMPLOYMENT, FROM, THROUGH, GROSS EARNINGS DURING WEEK PERIOD, HOURLY, WEEKLY, MONTHLY, NUMBER OF HOURS NORMALLY WORKED, NUMBER OF DAYS NORMALLY WORKED PER, DATES ABSENT FOLLOWING ACCIDENT, HAS EMPLOYEE RECEIVED IS EMPLOYEE, YES, UNDETERMINED, and WORKERS COMPENSATION INSURER box.
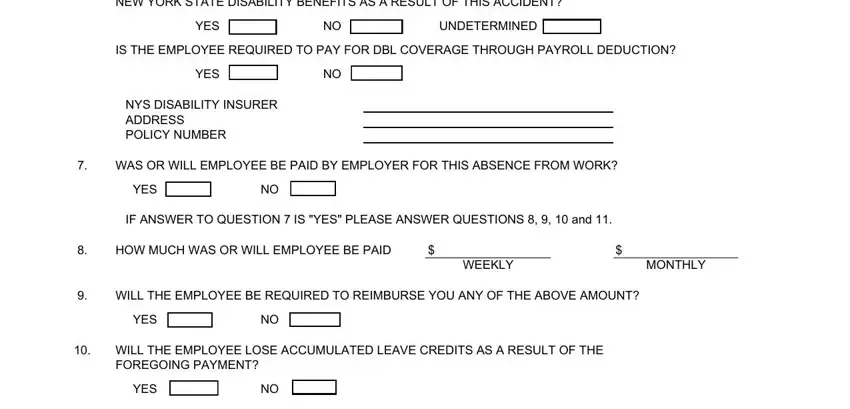
You'll be asked to enter the details to help the system prepare the field HAS EMPLOYEE RECEIVED IS EMPLOYEE, YES, UNDETERMINED, IS THE EMPLOYEE REQUIRED TO PAY, YES, NYS DISABILITY INSURER ADDRESS, WAS OR WILL EMPLOYEE BE PAID BY, YES, IF ANSWER TO QUESTION IS YES, HOW MUCH WAS OR WILL EMPLOYEE BE, WEEKLY, MONTHLY, WILL THE EMPLOYEE BE REQUIRED TO, YES, and WILL THE EMPLOYEE LOSE ACCUMULATED.
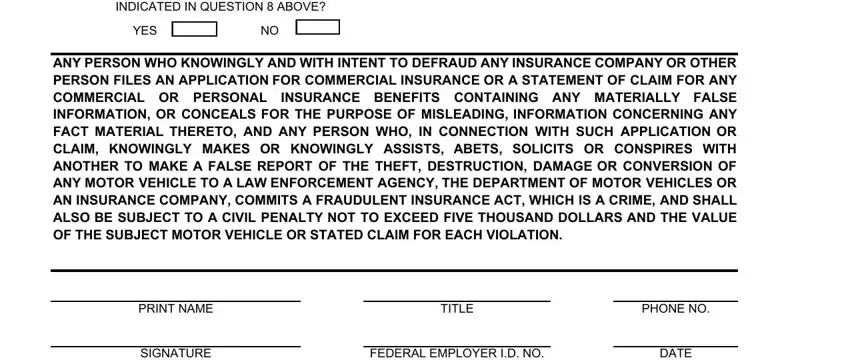
Within the box WILL THE EMPLOYEES ELIGIBILITY FOR, YES, ANY PERSON WHO KNOWINGLY AND WITH, PRINT NAME, TITLE, PHONE NO, SIGNATURE, FEDERAL EMPLOYER ID NO, and DATE, write down the rights and responsibilities of the parties.
Step 3: Hit the "Done" button. Finally, you can transfer the PDF file - save it to your device or send it by using email.
Step 4: Generate a duplicate of every different form. It may save you time and make it easier to avoid difficulties later on. By the way, your details isn't going to be distributed or viewed by us.
